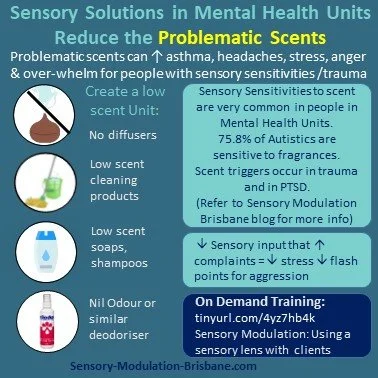
Low scent, fragrances in Mental Health Unit Design
The prevalence of fragrance sensitivities were investigated in the United States, United kingdom, Australia and Sweden by Steinemann (2019) and results included:
· 75.8% of Autistics are sensitive to fragrances
· 26% of the general population report being diagnosed with asthma/asthma like conditions and 57.8% are also fragrance sensitive.
Scents that were particularly problematic included:
· Air fresheners and deodorisers (54.8%)
· Being in a room with recently cleaned products (53.8%)
· Being near someone wearing a fragranced product (56.5%)

Low Scent, Fragrances in Mental Health Unit Design
This blog will outline the rationale for a low scent environment in Mental Health Units and offer recommendations with respect to the design of these environments.
People admitted to Mental Health inpatient Units present with a wide range of mental health disorders including schizophrenia, Borderline Personality Disorder, Post Traumatic Stress Disorder and Autism Spectrum Disorder. It is now understood that people with these diagnoses experience a higher rate of sensory sensitivities and other sensory processing challenges compared to the general population (Stromberg et al).
The prevalence of fragrance sensitivities were investigated in the United States, United kingdom, Australia and Sweden by Steinemann (2019) and results included:
· 75.8% of Autistics are sensitive to fragrances
· 26% of the general population report being diagnosed with asthma/asthma like conditions and 57.8% are also fragrance sensitive.
Scents that were particularly problematic included:
· Air fresheners and deodorisers (54.8%)
· Being in a room with recently cleaned products (53.8%)
· Being near someone wearing a fragranced product (56.5%)
There was a range of adverse health effects associated with fragranced product exposures for chemically sensitive individuals and this included:
· Respiratory problems (50.2%)
· Mucosal symptoms (39.4%)
· Migraine headaches (36.9%)
· Asthma attacks (25.2%)
Scent was identified as a barrier to engaging in occupations including:
· 37.4% are unable or reluctant to use public restrooms that have an air freshener, deodoriser or scented product.
· 51% enter a business but then leave as quickly as possible due to a fragranced product
· 9% of the general population has lost work days or lost a job in the past year due to illness from fragranced product exposure in the workplace
· 60% of students in one study had a physical reaction including headaches, shortness of breath, or a rash after being exposed to fragranced products. Additionally, 41% noted their reactions to fragranced products impacted their ability to concentrate on studying and taking exams. (Lee, 2019)
Healthcare
· 51.45% of the general population would prefer that healthcare facilities and healthcare professionals are fragrance free.
· 77.2% of Autistics would prefer fragrance free healthcare.
PTSD:
Herz (2021) found that odors may be the most incapacitating triggers for PTSD because:
“ (1) odors are invisible and there is often no way to prepare for or anticipate the possibility of exposure;
(2) odors evoke more emotional and evocative memories than other sensory stimuli
(3) odors are processed in the area of the brain where emotions, emotional memories, and associations are processed (the amygdala-hippocampal complex and orbitofrontal cortex), which comprises the same neural circuitry as PTSD due to their direct connection to the neural network of emotion, odors can instantly elicit affective responses and associations prior to and without cognitive appraisal That is, at-risk individuals are vulnerable to traumatic odor-triggered memories; odor processing inherently elicits highly emotionally charged memories; and, due to the automaticity of odor-evoked memories, encountering an odor associated with trauma can sideswipe cognitively prepared coping responses.
In addition to being highly insidious triggers, odors often play a central role in PTSD episodes. For example, in a report of 100 refugees who were seen at a psychiatric clinic, 45 percent reported experiencing an odor-triggered panic attack within the preceding month [51]. Odor cues can also trigger particularly negative flashbacks.”
Sensory Modulation Brisbane recommends that Mental Health Units respond to the needs of people with sensory sensitivities and trauma triggers to scents by implementing sensory modulation techniques and Universal Health Design features such as:
· Availability of Nil Odor, Stink Balm or other odor reducing strategies to provide an option for people to decrease a scent that they do not like.
· Providing personally preferred scent input eg options for different soaps, little containers with cotton balls and scent on it.
· Low scent cleaning , laundry and bathroom products
· No aromatherapy diffusers, incense etc
· Scents to be considered as a possible contributor for distress and agitation.
· Problem solving to address scents that are identified as problematic by people on the ward
· Designing spaces to separate the food areas to keep food scents in one location.
· Consideration of separate eating areas or other strategies for people with scent sensitivities or triggers or who need lower scent levels in order to comfortably eat.
· Healthcare professionals to wear low scent personal products.
· Air purifiers, plants
· Open windows and outdoor areas
· Completing a personal safety plan to identify useful and problematic scents
Further information on this topic is available on the On demand course:
References:
S. Herz R. Olfactory Virtual Reality: A New Frontier in the Treatment and Prevention of Posttraumatic Stress Disorder. Brain Sciences. 2021; 11(8):1070. https://doi.org/10.3390/brainsci11081070
Lee, R., Westmoreland, D., Maju, M., Apolloni, A., Bullock, H., Wang, A., & Sidhu, S. (2019, November). Assessing the Prevalence of Chemical Sensitivities to Fragranced Products Among Undergraduate Students & Its Impact on Educational Experiences. In APHA's 2019 Annual Meeting and Expo (Nov. 2-Nov. 6). APHA.
Sensory Modulation Resource Manual
Steinemann, A. International prevalence of chemical sensitivity, co-prevalences with asthma and autism, and effects from fragranced consumer products. Air Qual Atmos Health 12, 519–527 (2019). https://doi.org/10.1007/s11869-019-00672-1
https://link.springer.com/article/10.1007/s11869-019-00672-1
Steinemann, A. The fragranced products phenomenon: air quality and health, science and policy. Air Qual Atmos Health 14, 235–243 (2021). https://doi.org/10.1007/s11869-020-00928-1
https://link.springer.com/article/10.1007/s11869-020-00928-1#citeas
Maria Strömberg, Lina Liman, Peter Bang, and Kajsa Igelström.Experiences of Sensory Overload and Communication Barriers by Autistic Adults in Health Care Settings.Autism in Adulthood.Mar 2022.66-75.http://doi.org/10.1089/aut.2020.0074
https://www.abc.net.au/news/2023-01-09/too-many-smelly-candles-here-s-how-scents-impact-the-air-quality/101823806

Therapy rooms and waiting rooms: designing for sensory needs
At Sensory Modulation Brisbane, we have been advocating for Universal Design in Mental Health Units for Sensory Sensitivities and we would recommend that this is expanded to therapy rooms, waiting rooms and all health care spaces.
Many people who attend Therapy practices have sensory processing patterns that are more sensitive, more avoiding, or more seeking or more missing of sensations than others and this can vary between different senses. This includes:
· Autistics have sensory processing differences recognised as a diagnostic criteria. (DSM5)
· People with PTSD often have reactivity and hypervigilance to certain sensations
· People with schizophrenia often have auditory processing and visual perception challenges.
· ADHDers frequently have sensory processing differences (Schulze 2020)
· A high percentage of people with mental illness have interoceptive difficulties
Therapy room with grey lounge, green cushions, a white blanket and a plant on a small table. We would remove the aromatherapy sticks though!
At Sensory Modulation Brisbane, we have been advocating for Universal Design in Mental Health Units for Sensory Sensitivities and we also recommend this for therapy rooms, waiting rooms and all health care spaces.
Many people who attend Therapy practices have sensory processing patterns that are more sensitive, more avoiding, or more seeking or more missing of sensations than others and this can vary between different senses. This includes:
· Autistics have sensory processing differences recognised as a diagnostic criteria. (DSM5)
· People with PTSD often have reactivity and hypervigilance to certain sensations
· People with schizophrenia often have auditory processing and visual perception challenges.
· ADHDers frequently have sensory processing differences (Schulze 2020)
· A high percentage of people with mental illness have interoceptive difficulties
It can be useful to design for people with sensory sensitivities as it is easier to add sensory input if needed rather than take it away.
Lighting
· Ideally a dimmable light that is set at the preference level of an individual client
· Curtains or Blinds to block out light
· If there is a florescent light, turn it off and use lamps instead.
Sound
· Improving office acoustics can be very beneficial for everyone in terms of privacy and also reducing distractions and sensory sensitivities and overload.
· It is preferable to not use music in a waiting room environment as people who want music can usually access this on their phone.
Scent
· Scents can be a trauma trigger, allergy trigger or lead to sensory sensitivity and overload. So having a low scent therapy room and waiting room can be very important. For this reason, we do not recommend diffusers in public spaces.
· Sometimes it may be necessary to neutralise odours. Try nil odour drops.
Interoception needs
Sometimes therapy is the place where people relax a little and notice that they need to go to the toilet, drink some water or have some snacks. They may not have noticed these interoceptive needs earlier. Close proximity to toilets, water and food can be useful.
Comfortable Seating
There are many people in pain or who have hypermobility and are attending therapy offices. Comfortable seating can make a big difference.
Calming tools
At Sensory Modulation Brisbane, our favourite sensory tools for offices including a weighted cushion, a box of fidgets, icy water or ice packs and invitations to reduce the lighting or turn on or off the pink/brown/white noise machine.
Visual Movement
Ideally design waiting rooms so that there is not a lot of visual movement eg people walking past, traffic etc. Or provide options to be able to not face this visual movement.
Clear Pathways
It is useful for pathways to be clear and obvious and for signage to be clear. It can also be useful to take pictures of landmarks and have this available on website or new starter information .
Personal preferences
It can be useful to invite individuals to use their preferred fidgets, earplugs, sunglasses, back cushion etc so that they are comfortable
Nature
Access to nature can be calming. A plant or a picture of nature can be good additions to an office
Previous blog posts have discussed changing sensory input within a psychiatric hospital:
Training:
https://sensorymodulationbrisbane.ticketspice.com/sensory-modulation-using-a-sensory-lens-with-clients
References:
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Marcel Schulze, Silke Lux, Alexandra Philipsen et al. Sensory Processing in Adult ADHD – A Systematic Review, 10 September 2020, PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-71514/v1]
chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://assets.researchsquare.com/files/rs-71514/v1/d616340b-9b38-4732-b56f-7c249e0632f7.pdf?c=1631855030
Sugiyama, S., et al(2021). The Auditory Steady-State Response: Electrophysiological Index for Sensory Processing Dysfunction in Psychiatric Disorders. Frontiers in psychiatry, 12, 644541.
Sensory Modulation Resource Manual

Sensory Kits , Trauma Informed Practice and NDIS
Using Sensory items to calm and ground are recognized evidence based strategies.
Yet some people in the NDIS scheme are having NDIS Plan Managers refuse to fund sensory items
This blog provides a rationale for the NDIS to make changes to their website and price guide based on two guidelines.
1. The Disability Guidelines for Trauma –Informed Practice: Supporting people with disability who have experienced complex trauma
2. NDIS Quality and Safeguards Commission (2020) Regulated Restrictive Practices Guide

Using Sensory items to calm and ground are recognized evidence based strategies.
Yet some people in the NDIS scheme are having NDIS Plan Managers refuse to fund sensory items
This blog provides a rationale for the NDIS to make changes to their website and price guide based on two guidelines.
1. The Disability Guidelines for Trauma –Informed Practice: Supporting people with disability who have experienced complex trauma
2. NDIS Quality and Safeguards Commission (2020) Regulated Restrictive Practices Guide
The Disability Guidelines for Trauma-Informed Practice: Supporting people with disability who have experienced complex trauma were developed in response to the disability royal commissions findings of high numbers of cases of abuse against people with disability. In response, the government provided funding for the project to develop the Disability Guidelines for Trauma-Informed Practice:
“The Morrison government is backing the creation of a best-practice guide to help the disability sector better support people with disability who have experienced complex trauma.
Social Services Minister Anne Ruston said the government was investing $267,760 in the project to ensure Australia leads the way in supporting people with disability who suffer violence, abuse, neglect or exploitation.
“The Morrison government will fund Blue Knot Foundation to guide organisations and practitioners on how to better understand complex trauma and deliver trauma-informed care to the disability community,” Ruston said.”
(Probono Australia) https://probonoaustralia.com.au/news/2020/08/new-guide-to-help-build-a-trauma-informed-disability-sector/
Within the Disability Guidelines for Trauma-Informed Practice , there is a section on developing comfort kits:
“Before the person needs grounding and if the person is able:
• Locate something that the person finds calming to look at.
• Locate something that the person finds calming to listen to.
• Locate something that the person likes to touch.
• Locate something that the person likes to smell.
• Locate something that the person likes to taste.
Place all of these items in a box. When triggered encouraged the person to access their box and use the five senses to explore each item until they can return to the Window of Tolerance.”
If a person is in the Window of Tolerance it means that they are able to concentrate and engage in activities. (Being outside the window of tolerance includes being stressed or shutdown)
Another guideline which is also supportive of developing comfort kits and sensory items is the NDIS Quality and Safeguards Commission (2020) Regulated Restrictive Practices Guide.
Examples of using sensory items to calm include:
Participant “having a quiet space in her home with sensory and relaxation items”. P 38
Participant having a sensory room that was designed for her sensory needs. “this included different items and activities, some of which were portable and could be used within the community when she needed them……The sensory room was to be used proactively to assist Emma to feel calm when she was beginning to show early signs of distress. P 55 and 56
Despite these guidelines having clear support for the provision of sensory items for people with disabilities, it is something that many participants find that it is difficult to obtain funding for.
Solution: NDIS to change the " would we fund it page" and/or develop a line item in their price guide to support people with disabilities and trauma

Auditory Processing Needs in Mental Health Unit Design
This blog will outline the auditory sensitivities and sensory processing challenges of people admitted to Mental Health Units and offer recommendations with respect to the design of these environments.
People admitted to Mental Health inpatient Units present with a wide range of mental health disorders including schizophrenia, Borderline Personality Disorder, Post Traumatic Stress Disorder and Autism Spectrum Disorder. It is now understood that people with these diagnoses experience a higher rate of sensory sensitivities and other sensory processing challenges compared to the general population (Stromberg et al).
The sensory system we will focus on today is the Auditory system.
Auditory Processing difficulties have been recognised and explored across a range of research areas including:
Occupational Therapy research of sensory processing difficulties (eg Harrison et al)
Lived experience research such as Autistics, people with schizophrenia (eg Stromberg et al)
Neuroscience research of Auditory State Response gating (eg Sugiyama et al )
Diagnostic Criteria such as hypervigilance to sounds in PTSD and sensory over-responsivity in Autism Spectrum Disorder.

This blog will outline the auditory sensitivities and sensory processing challenges of people admitted to Mental Health Units and offer recommendations with respect to the design of these environments.
People admitted to Mental Health inpatient Units present with a wide range of mental health disorders including schizophrenia, Borderline Personality Disorder, Post Traumatic Stress Disorder and Autism Spectrum Disorder. It is now understood that people with these diagnoses experience a higher rate of sensory sensitivities and other sensory processing challenges compared to the general population (Stromberg et al).
The sensory system we will focus on today is the Auditory system.
Auditory Processing difficulties have been recognised and explored across a range of research areas including:
Occupational Therapy research of sensory processing difficulties (eg Harrison et al)
Lived experience research such as Autistics, people with schizophrenia (eg Stromberg et al)
Neuroscience research of Auditory State Response gating (eg Sugiyama et al )
Diagnostic Criteria such as hypervigilance to sounds in PTSD and sensory over-responsivity in Autism Spectrum Disorder.
Sensory Modulation Brisbane recommends that Mental Health Units respond to the needs of people with auditory processing difficulties by implementing sensory modulation techniques and Universal Health Design features such as:
Availability of earplugs, headphones, other devices for reducing sounds (eg white/brown/pink noise machines) or providing personally preferred input
Sound proofing, acoustic consultants and co-design by Autistics and others with lived experience.
No fluorescent lights (due to the sounds)
No ticking clocks
Alarms on the unit be either visual or vibration or sound is reduced in some way.
Allocated spaces on the ward with lower sound levels
Allocated spaces on the ward where people can listen to preferred sound
Sound to be considered as a possible contributor for distress and agitation.
Problem solving to address sounds that are identified as problematic by people on the ward
Consideration of separate eating areas or other strategies for people with misophonia (unable to stand sounds of others eating) or who need lower sound levels in order to comfortably eat.
Consideration of background sound when speaking with someone on the ward
Further information on this topic is available on the On demand course:
References:
Harrison LA, Kats A, Williams ME, Aziz-Zadeh L. The Importance of Sensory Processing in Mental Health: A Proposed Addition to the Research Domain Criteria (RDoC) and Suggestions for RDoC 2.0. Front Psychol. 2019 Feb 5;10:103. doi: 10.3389/fpsyg.2019.00103. PMID: 30804830; PMCID: PMC6370662.
Maria Strömberg, Lina Liman, Peter Bang, and Kajsa Igelström.Experiences of Sensory Overload and Communication Barriers by Autistic Adults in Health Care Settings.Autism in Adulthood.Mar 2022.66-75.http://doi.org/10.1089/aut.2020.0074
Sugiyama S, Ohi K, Kuramitsu A, Takai K, Muto Y, Taniguchi T, Kinukawa T, Takeuchi N, Motomura E,
Nishihara M, Shioiri T and Inui K (2021) The Auditory Steady-State Response: Electrophysiological Index for Sensory Processing Dysfunction in Psychiatric Disorders. Front. Psychiatry 12:644541. doi: 10.3389/fpsyt.2021.644541
Sensory Modulation to reduce restrictive practice Part 2: Policy Context
Currently, NDIS providers are struggling to reduce the use of restrictive practices in service delivery. A report by the NDIS Quality and Safeguards Commission showed that there were more than a one million incidents of unauthorised restraints in 2020 – 2021, a 240% increase from the previous 12 months. The restraints included use of sedation, strapping down a person or depriving them of their personal belongings. (Henriques-Gomes, 2021 report of NDIS quality and safeguards commission)
As described in Part 1 of this blog series, Sensory Modulation is an intervention shown to be effective for reducing restrictive practice. Sensory Modulation can be defined as “using your senses to change the way you feel” (O’ Sullivan, Fitzgibbon 2017). Sensory Modulation interventions involve:
identifying problematic, or overwhelming sensory stimuli and developing strategies to reduce the input or promote self-regulation, with the goal of supporting the individual to continue to be able to engage in occupations.
Identifying calming and soothing sensory strategies to prevent the use of and/or be an alternatives to restrictive practices.
Currently, NDIS providers are struggling to reduce the use of restrictive practices in service delivery. A report by the NDIS Quality and Safeguards Commission showed that there were more than a one million incidents of unauthorised restraints in 2020 – 2021, a 240% increase from the previous 12 months. The restraints included use of sedation, strapping down a person or depriving them of their personal belongings. (Henriques-Gomes, 2021 report of NDIS quality and safeguards commission)
As described in Part 1 of this blog series, Sensory Modulation is an intervention shown to be effective for reducing restrictive practice. Sensory Modulation can be defined as “using your senses to change the way you feel” (O’ Sullivan, Fitzgibbon 2017). Sensory Modulation interventions involve:
identifying problematic, or overwhelming sensory stimuli and developing strategies to reduce the input or promote self-regulation, with the goal of supporting the individual to continue to be able to engage in occupations.
Identifying calming and soothing sensory strategies to prevent the use of and/or be an alternatives to restrictive practices.
Sensory Modulation can incorporate individual and group interventions and changing sensory spaces including lowered stimulus, increased sensory stimulation and specifically designed rooms known as sensory or comfort rooms. Sensory Modulation can occur in any environment, and is optimally delivered by trained staff or through a care-plan designed by an occupational therapist. Sensory modulation strategies can be used in the person’s home or in the community, in group living environments, or in dedicated space such as Snoezelen rooms or multisensory environments anywhere where the person has control over the sensory input to accommodate their unique sensory preferences.
The following case study illustrates the implementation of sensory modulation strategies in a mental health inpatient setting.
Note: Trigger warning for this article as behaviours of concern are discussed, such as self harm and restrictive practices.
Marsha has been in a mental health unit for 3 months. While she was in hospital she had access and learnt to use Sensory Modulation strategies when she had urges to self harm. Marsha found these much more useful than taking medication. Marsha had previously experienced episodes where she had been chemically restrained by her support workers, and felt access to sensory modulation strategies would offer a better alternative in the future. As part of her discharge planning, Marsha agreed it would be helpful to include sensory modulation strategies to enable her to safely transition home, and she also stated that it would be helpful for her to purchase a weighted blanket for calming, as well as some scents. Marsha had identified that one of the triggers for an urge to self harm was the smell of tobacco, as this reminded her of a traumatic situation in her past. Marsha had learnt that if she regularly applied a scent to her handkerchief and held it up to her nose, she could tolerate being around the tobacco without urges to self harm and even wait at the bus stop for her bus to TAFE.
Marsha’s plan manager explained that the NDIS do not fund sensory items and Marsha was unable to purchase the weighted blanket and scents.
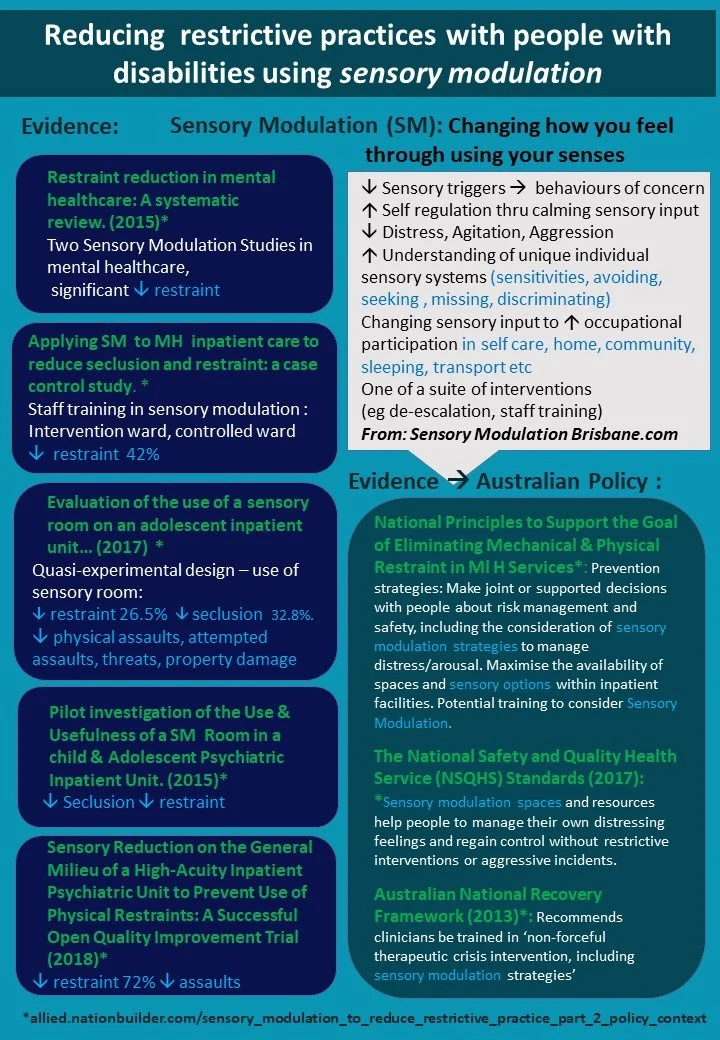
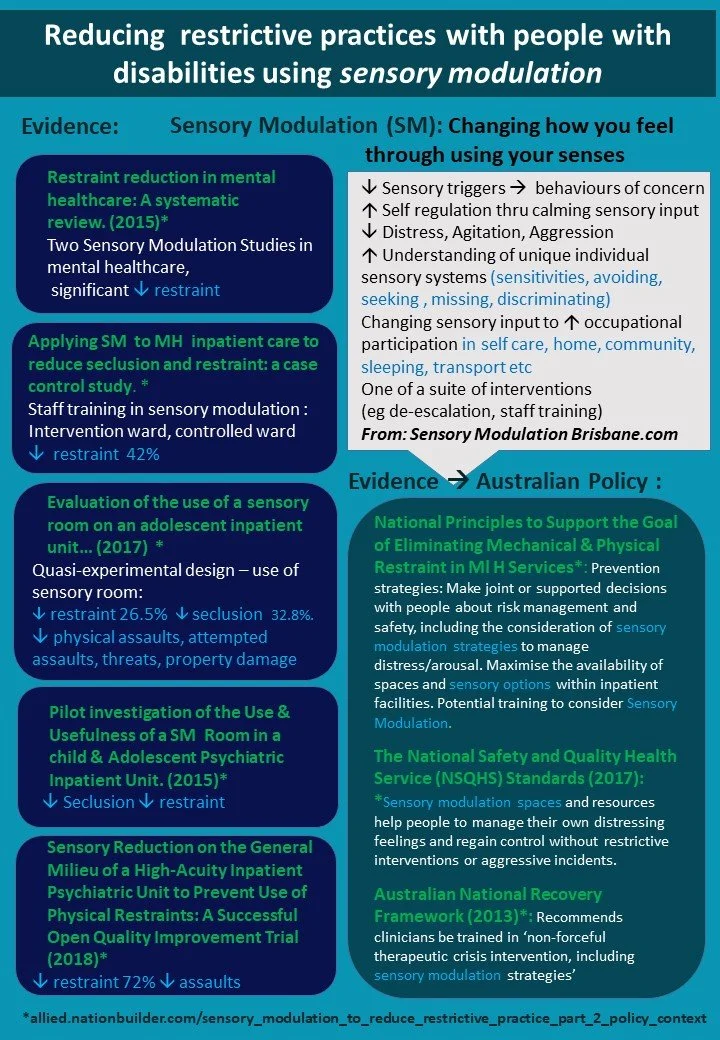
In this case study Marsha was using Sensory Modulation interventions on a Mental Health Unit. Sensory Modulation is a common intervention in Australian Mental Health Services and has extensive policy support as a strategy to reduce Seclusion and Restraint in Mental Health Units. Both national and State-level policy frameworks that support Sensory Modulation in mental health settings, are listed in detail in the ‘Where can I learn more?’ section below.
In the disability context, the NDIS Quality and Safeguards Commission (2020) Regulated Restrictive Practices Guide highlights support for sensory interventions directly such as sensory rooms and sensory items, as well as indirect support such as recommending identifying and removing potential triggers and identifying environmental changes which could include changes to the sensory aspect of the environment. For example, this document states (bold text added for emphasis):
“Consideration should be given to the physical environment of the seclusion area and any items that can be offered to ensure the person has appropriate sensory input, subject to a risk assessment (Mckenna et al, 2014 cited in NDIS commission report)” P.28
“Some of the strategies aimed to increase Sue’s quality of life and help support the medication reduction plan and reduce the incidents of chemical restraint focused on:
"Having a quiet space in her home with sensory and relaxation items.” P.38
“Some of the strategies aimed to increase Emma’s quality of life and help support the reduction and elimination of seclusion focuses on:
A Sensory room was designed for Emma tailored to her sensory needs. It included different items and activities, some of which were portable and could be used within the community when she needed them. Over time, it was hoped that having a sensory room would replace the use of seclusion. The sensory room was to be used proactively to assist Emma to feel calm when she was beginning to show early signs of distress.” P. 55 & 56
Despite NDIS Quality and Safeguards Commission (2020) Regulated Restrictive Practices Guide highlighting support for sensory interventions, there continues to be challenges in ensuring these interventions are funded for people with disabilities through NDIS plans, for the purpose of reducing restrictive practice. These challenges include a lack of awareness of the benefits of Sensory Modulation on the part of NDIS planners. In addition, NDIS Guidelines indicate that sensory items will not be funded for children with autism or developmental delay – and this guideline is often interpreted as sensory interventions broadly -including Sensory Modulation strategies – are not likely to be funded. Many occupational therapists are concerned that a proven intervention with capacity to reduce restrictive practice, is currently overlooked in the NDIS space - while rates of restrictive practice, are growing exponentially.
It is hoped that the NDIS Quality and Safeguards Commission will advocate for further sensory modulation options to be funded to support the reduction of restrictive practices for people with disabilities.
What could this mean for day-to-day work?
Allied health professionals trained to provide sensory modulation interventions can provide person centred and tailored strategies to reduce the need for restrictive practice for people with disabilities.
How can I influence change?
Raise awareness of the strong evidence-base and policy context for sensory modulation interventions through sharing with colleagues, policymakers and funding bodies.
Authors: Carolyn Fitzgibbon and Julie O’Sullivan
Carolyn and Julie are co-authors of the Sensory Modulation Resource Manual and co-directors of Sensory Modulation Brisbane.
References:
Helene Andersson, Daniel Sutton, Ulrika Bejerholm & Elisabeth Argentzell (2021) Experiences of sensory input in daily occupations for people with serious mental illness, Scandinavian Journal of Occupational Therapy, 28:6, 446-456, DOI: 10.1080/11038128.2020.1778784
Andersen, Kolmos, A., Andersen, K., Sippel, V., & Stenager, E. (2017). Applying sensory modulation to mental health inpatient care to reduce seclusion and restraint: a case control study. Nordic Journal of Psychiatry, 71(7), 525–528. https://doi.org/10.1080/08039488.2017.1346142
Azuela, Gilbert (2019). The implementation and impact of sensory modulation in Aotearoa New Zealand adult acute mental health services: Two organisational case studies
Bailliard and Whigham’s (2017 cited in Wilson 2020) scoping review of 149 studies on Sensory Processing and mental illness found that interventions targeting sensory processing skills such as sensory rooms may contribute to cognitive gains and improve occupational performance.
Brown, C., Stoffel, V., & Munoz, J. P. (2011). Occupational therapy in mental health: A vision for participation. Philadelphia: F.A. Davis Co. Chapter 22 Catana Brown, Patricia Steffen-Sanchez and Rebecca Nicholson
Champagne,T (2018) Sensory Modulation in Dementia Care: Assessment and Activities for Sensory-enriched Care, Jessica Kingsley Publishers, London, 2018, 168 pp., pbk £15.99, ISBN 13: 9781785927331. - Volume 39 Issue 8
Dorn, Emma, Hitch, Danielle and Stevenson, Christopher 2020, An evaluation of a sensory room within an adult mental health rehabilitation unit, Occupational therapy in mental health, vol. 36, no. 2, pp. 105-118, doi: 10.1080/0164212X.2019.1666770.
Im D. S. (2021). Treatment of Aggression in Adults with Autism Spectrum Disorder: A Review. Harvard review of psychiatry, 29(1), 35–80. https://doi.org/10.1097/HRP.0000000000000282
Henriques-Gomes, L. 10 Nov, 2021 Guardian Australia
MacLennan, K., O’’ Brien, S., and Tavassoli, T (2021) In our Own Words: The Complex Sensory Experiences of Autistic Adults. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-021-05186-3
O’Sullivan, J and Fitzgibbon, C. (2017) Sensory Modulation Resource Manual.
Matson, R., Kriakous, S and Stinson, M (2021) The Experiences of Women with a Diagnosis of Borderline Personality Disorder (BPD) Using Sensory Modulation Approaches in an Inpatient Mental Health Rehabilitation Setting, Occupational Therapy in Mental Health, 37:4, 311-331, DOI: 10.1080/0164212X.2021.1933674
NDIS Quality and Safeguards Commission (2020).Regulated Restrictive Practices Guide. Penrith. Australia: NDIS Quality and Safeguards Commission.
Seckman, Angela ; Paun, Olimpia ; Heipp, Biljana ; Stee, Marie ; Keels‐Lowe, Vonda ; Beel, Frank ; Spoon, Cari ; Fogg, Louis ; Delaney, Kathleen R, Evaluation of the use of a sensory room on an adolescent inpatient unit and its impact on restraint and seclusion prevention Journal of child and adolescent psychiatric nursing, 2017-05, Vol.30 (2), p.90-97
Tavassoli, T., Bellesheim, K., P, M,. Wang, A. T., Halpern, D., Gorenstein, M., Grodberg, D., Kolevzon, A., and Buxbaum, J.D. (2016) Measuring Sensory Reactivity in Autism Specrum Disorder: Application and Simplification of a Clinician-Administered Sensory Observation Scale. Journal of Autism and Developmental Disorders, 46 (1), 287 – 293. Hyyps://doi.org/10.1007/s10803-015-2578-3
Van den Boogert F, Sizoo B, Spaan P, Tolstra S, Bouman YHA, Hoogendijk WJG, Roza SJ. (2021) Sensory Processing and Aggressive Behavior in Adults with Autism Spectrum Disorder. Brain Sci. 14;11(1):95. doi: 10.3390/brainsci11010095. PMID: 33466570; PMCID: PMC7828723.
Verhulst, I., MacLennan, K., Haffey, A., & Tavassoli, T. (2022, January 12). The perceived casual relations between sensory reactivity differences and anxiety symptoms in autistic adults.
Unwin, K. L., Powell, G., & Jones, C. R. (2021). The use of Multi-Sensory Environments with autistic children: Exploring the effect of having control of sensory changes. Autism. https://doi.org/10.1177/13623613211050176
Werkman, M.F., Landsman, J.A., Fokkens, A.S. et al. (2022) The Impact of the Presence of Intellectual Disabilities on Sensory Processing and Behavioral Outcomes Among Individuals with Autism Spectrum Disorders: a Systematic Review. Rev J Autism Dev Disord https://doi.org/10.1007/s40489-022-00301-1
Wilson, Haley, "Mental Health Inpatient Hospitalization: What Nursing Can Learn From "Sensory Rooms."" (2020). Honors Theses. 3315. https://scholarworks.wmich.edu/honors_theses/3315
Wright, L. Bennett, S, Meredith, P (2020) ‘Why didn't you just give them PRN?’: A qualitative study investigating the factors influencing implementation of sensory modulation approaches in inpatient mental health units https://doi-org.ezproxy.library.uq.edu.au/10.1111/inm.12693
Zeanah, C. (2018) Handbook of Infant Mental Health Fourth edition. Chapter 19: Sensory Over-responsivity Timothy W Soto, Vivian Ciaramitaro, Alice Carter.
Zimmermann, D. P. S. (2020). Use of a serenity room for sensory modulation (Order No. 28002838). Available from ProQuest Dissertations & Theses Global. (2420652212). https://www.proquest.com/dissertations-theses/use-serenity-room-sensory-modulation/docview/2420652212/se-2?accountid=14723
Australian National Policies, Reports and Frameworks that contain references to Sensory Modulation, Sensory Items, Sensory Rooms or Sensory Approaches.
NDIS QUALITY & SAFEGUARD COMMISSION (2020) Regulated Restrictive Practices Guide
National Mental Health Commission
National Principals to Support the Goal of Eliminating Mechanical and Physical Restraint in Mental Health Services (Mental Health Commission)
Australian National framework for recovery-oriented mental health services: Guide for practitioners and providers (2013)
State Policies, Reports and Frameworks that contain references to Sensory Modulation, Sensory Items, Sensory Rooms or Sensory Approaches.
Mental Health Act 2016 Chief Psychiatrist Policy Mechanical Restraint, QLD (2020) :
Mental Health Act 2016 Chief Psychiatrist Policy Physical Restraint, QLD (2020) :
Admission of children and adolescents to acute mental health inpatient units – Queensland Health Guideline (2021)
Suicide Prevention Health Taskforce – Phase 1 Action Plan (2017) Qld Health
Mental Health Safety and Quality NSW
Chief Psychiatrist Restraint and Seclusion Standard A standard to reduce and eliminate where possible the use of restraint and seclusion applied under the Mental Health Act 2009 (2021) South Australia:
South Australia Policy: Guideline Restraint and Seclusion in Mental Health Services Policy Guideline
Health framework for reducing restrictive interventions Victoria: Victoria Positive Practice Framework
Attachment and Trauma in People with an Intellectual Disability (2008), Positive Solutions in Practice, Office of the Senior Practitioner.
Mental Health Restraint Policy West Australia(2020) West Australia Prevention and early intervention strategies
Sensory Modulation to reduce restrictive practice Part 1: Evidence base
In part 1 of this 2-part series, the current evidence for using Sensory Modulation will be discussed. A fictional case study will highlight these issues. Note: Trigger warning for this article as behaviours of concern are discussed, such as self harm and restrictive practices.
Sensory Modulation for Self-Regulation
Sensory modulation approaches involve the provision of sensory-based therapy tools and/or the creation of appropriate environments that engage the user’s senses to reduce the build-up of agitation and prevent the escalation of aggression (eg Chalmers et al 2012, Lee et al 2010). (O Sullivan and Fitzgibbon, 2017).

Carolyn and Julie wrote a guest blog on the allied.org.au website. This organisation is an advocacy organistion and very worthwhile to join. There is a mailing list for more articles and blogs on a range of allied health topics, including NDIS. This is a new website hoping to share many allied health and lived experience perspectives.
In part 1 of this 2-part series, the current evidence for using Sensory Modulation will be discussed. A fictional case study will highlight these issues. Note: Trigger warning for this article as behaviours of concern are discussed, such as self harm and restrictive practices.
Sensory Modulation for Self-Regulation
Sensory modulation approaches involve the provision of sensory-based therapy tools and/or the creation of appropriate environments that engage the user’s senses to reduce the build-up of agitation and prevent the escalation of aggression (eg Chalmers et al 2012, Lee et al 2010). (O Sullivan and Fitzgibbon, 2017).
A significant driving force for services to adopt sensory modulation was the need to develop ‘alternative methods for managing distress, agitation and aggressive behaviour’ (O’Hagan, 2006) including to reduce seclusion and restraint practices.
Sensory Modulation is useful when there is a sensory trigger to a behaviour of concern, and then a sensory solution can be applied to reduce or minimise the sensory input. (eg using noise cancelling headphones to reduce overwhelming noise).
A sensation can act as a trigger due to a number of reasons including a past memory or traumatic association, intense dislike of a sensation or due to a person experiencing sensory overload or reaching their tolerance for sensory input as part of a hypersensitivity. In some individuals, the intense need to avoid the sensation can lead to a behaviour of concern (eg running away from the sensation, pushing a person away to avoid a sensation).
Verhulst et al (2022) found that “Visual, auditory and olfactory hyper reactivity, such as difficulties with bright, or flickering lights, sudden loud noises, and intense scents, have been commonly reported by autistic individuals and are associated with distress, overwhelm, and anxious responses. “ (MacLennan, et al 2021, Tavasolli et al 2016 cited in Verhulst et al 2022).
Sensory sensitivities are recognised in the Autism Spectrum Disorder diagnostic criteria and have also been found to be atypical in adults with schizophrenia, for example auditory sensitivities (eg Adler, Waldo and Freedman,1985,cited in Soto et al ) and visual and somatosensory sensitivities (Andrade, Butler, Peters, Molholm and Foxe 2016 cited in Soto et al). Other mental illness’ shown to have sensory processing differences include Bipolar, Depression, Post Traumatic Stress Disorder (PTSD) and Obsessive Compulsive Disorder (OCD) (Brown et al, 2011). Other disabilities with sensory processing dysfunction include Intellectual Disabilities (Werkmen et al 2022) and Dementia (Champagne, 2018).
It is also important to note that for those people who do not have sensory processing dysfunction normally, when acutely distressed may become oversensitive to input such as noise and bright light or under responsive to other input such as visual cues. (Andersson et al 2021).
Wright et al (2020), stated that “Evidence suggests that the use of sensory modulation approaches can reduce a person's emotional distress and agitation (Adams-Leask et al. 2018; Chalmers et al. 2012; Cummings et al. 2010; Lloyd et al. 2014 cited in Wright et al 2020).
Unwin et al (2021) described benefits for controlling sensory stimulation for autistic children and adults:
Interventions to control sensory stimulation in everyday environments have shown benefits for autistic children and adults, including the use of headphones (e.g. Ikuta et al., 2016; Pfeiffer et al., 2019; Rowe et al., 2011) and modification in lighting (e.g. Kinnealey et al., 2012). Across the studies, these adaptations led to a range of improvements in attention (Kinnealey et al., 2012; Pfeiffer et al., 2019; Rowe et al., 2011), meeting individualised goals (Ikuta et al., 2016), mood and classroom performance (Kinnealey et al., 2012), and reductions in anxiety and challenging behaviours (Pfeiffer et al., 2019). Kinnealey et al. (2012) also report some improvement in social interaction, although only after several weeks of intervention. These findings are consistent with teacher reports that increasing autistic children’s control over the classroom environment helps them control unwanted sensory experiences, and that it is the uncontrollable and unpredictable nature of sensory stimuli that causes the most difficulty for their learning (Jones et al., 2020).
Sensory Modulation can also be used to support an individual’s self regulation and increase coping strategies, even when there is not a sensory trigger or sensory aspect. Sensory Modulation may include using sensory input to provide regulation, distraction, calming, grounding or to achieve a lower or higher sensory stimulation.
Altering the environment by using calming features or moving to a less overwhelming context was the most common strategy reported for managing sensory overstimulation in Andersson et al 2021 study. However, for many people including frail, aged, and those living with disabilities, it can be difficult to move themselves to a different/more suitable environment due to a range of factors. Such factors may include mobility issues, comprehension or communication difficulties, socio-economic constraints, environmental constraints, dependence on others to meet personal care needs
Sensory Modulation for Reducing Seclusion and Restraint
Sensory Modulation is a common practice intervention in Australian Mental Health Services and has policy support as a strategy to reduce Seclusion and Restraint in Mental Health Units (refer to blog 2 for further information).
In the United States in 2006, the National Association of State Mental Health Program Directors (NASMHPD) developed six core strategies to reduce seclusion and restraint. These strategies have been implemented by many other countries including Australia, New Zealand, the United Kingdom and a number of European countries. One of the core strategies recommends the use of ‘de-escalation surveys or safety plans, use of person-first language, environmental changes to include comfort and sensory rooms; sensory modulation experiences and other meaningful treatment activities. These tools actively support people to develop emotional self-management skills’ (Huckshorn, et al 2006 cited in O’Sullivan and Fitzgibbon (2017).
The role of Sensory Modulation in reducing seclusion and restraint has been most researched within Mental Health Units and there are multiple studies to demonstrate its effectiveness. Studies include Andersen et al. 2017; Barton et al. 2009; Champagne & Stromberg 2004; Lloyd et al. 2014; Maguire et al. 2012; Sivak 2012; Yakov et al. 2017 cited in Wright et al , (2021) and Seckman et al (2017) Bobier et al (2015). More recently, Zimmerman’s 2020 study on the implementation of a serenity/comfort room for sensory modulation found a decrease in chemical restraint, seclusion and mechanical restraint. Azuela, (2019)Gilbert found that service users in a psychiatric unit reported that sensory modulation was preferred over in situ medication (PRN) as a calming strategy.
In a study by Van den Boogert (2021) autistic adults with higher scores in sensory sensitivity had the highest risk of aggressive behaviour and thus applying detailed diagnostics on sensory processing difficulties when treating aggressive behaviour was recommended.
Sensory Modulation has also been used to decrease self harm. In one study (Matson et al (2021) participants found that they were able to use sensory input to experience a sense of release that they would normally achieve from self harming, but without any different. This depended on the usual method of self harm and was different for each individual
Im (2021) reviewed treatment of Aggression in Adults with Autism Spectrum Disorder and found that both multisensory interventions and behavioural interventions had similar levels of evidence.
“Lower levels of evidence (e.g., nonrandomized N of 1 trials, prospective open trials, retrospective reviews) point to possible benefits, in adults with ASD and aggression, of behavioural interventions,56,57,67,85–88,91–95,99 multisensory environments,96,109 yokukansan,58,110 clomipramine,104 sertraline,46,103 clozapine,115,117 and aripiprazole.76,77,82,116 Among these interventions, multisensory environments and yokukansan are slightly more supported based on risk-of-bias assessments. While the level of evidence for these approaches is less robust than for controlled trials, the adverse effects and long-term risks associated with many of these treatments (in particular, behavioral interventions and multisensory environments) are significantly more favourable.”(Im, 2021)
In the area of dementia, there have been studies reporting a decrease in the number of behavioural and psychological symptoms with the use of multi sensory environments (Maseda et al., 2014a; Minner et al., 2004; Riley-Doucet & Dunn, 2013; Staal et al., 2007; Ward-Smith et al., 2009), cited in Unwin et al (2020).
Case Study: Bruce
Bruce was visiting the shops to buy groceries for dinner. He enjoyed cooking and was looking forward to preparing his favourite meal – chicken nuggets. When Bruce was walking through the shops, a nearby child starting having a tantrum, which involved screaming and lying on the shop floor. Bruce and his support worker quickly moved further away, but Bruce could still hear the noise and it was driving him crazy! He held his hands over his ears and started rocking on the floor. His support worker wanted to support Bruce to leave the shops and started pulling on his arm to go. Unfortunately the situation quickly deteriorated, with the support worker physically restraining Bruce in an attempt to stop him from running away from the shops. When Bruce got home he started banging his head, and rocking back and forth into the wall.
Bruce discussed this incident with his treating team and it was identified that the sound of the child screaming was a trigger for him. They identified the strategy of using noise cancelling headphones if Bruce was out and heard an overwhelming sound. Bruce had always enjoyed using his Aunty’s rocking chair and it was identified that this could be a useful calming strategy at home as an alternative to head banging.
Bruce’s Occupational Therapist wrote a supporting letter addressing reasonable and necessary criteria to enable Bruce to use his NDIS funds to purchase noise cancelling headphones and a rocking chair. Staff training was also completed on using sensory modulation interventions. Bruce felt positive regarding his new strategy and found that it worked well for him, both at the shops and at home, thus preventing the need for further restraint.
Sensory Modulation is one of a suite of interventions to reduce seclusion and restraint. As this case study highlights, it needs to be tailored to the individual and accompanied by staff training and verbal de-escalation strategies. The NDIS could increase their support of Sensory Modulation items and interventions as a strategy to reduce seclusion and restraint and decrease behaviours of concern. In light of recent evidence from the NDIS Quality and Safeguards Commission highlighting a concerning increase in the use of restrictive practices including physical and chemical restraint, there is a strong case for exploring alternatives to these practices, and as described in this article and case study, sensory modulation has potential to be a viable strategy to reduce restrictive practice in the NDIS context. Alongside reducing restrictive practice, sensory modulation can have a positive impact on the individual’s functioning and quality of life.
What could this mean for day-to-day work?
Allied health professionals trained to provide sensory modulation interventions can provide person centred and tailored strategies to reduce the need for restrictive practice for people with disabilities.
How can I influence change?
Raise awareness of the strong evidence-base and policy context for sensory modulation interventions through sharing with colleagues, policymakers and funding bodies.
Authors: Carolyn Fitzgibbon and Julie O’Sullivan
Carolyn and Julie are co-authors of the Sensory Modulation Resource Manual and co-directors of Sensory Modulation Brisbane.
References:
Helene Andersson, Daniel Sutton, Ulrika Bejerholm & Elisabeth Argentzell (2021) Experiences of sensory input in daily occupations for people with serious mental illness, Scandinavian Journal of Occupational Therapy, 28:6, 446-456, DOI: 10.1080/11038128.2020.1778784
Andersen, Kolmos, A., Andersen, K., Sippel, V., & Stenager, E. (2017). Applying sensory modulation to mental health inpatient care to reduce seclusion and restraint: a case control study. Nordic Journal of Psychiatry, 71(7), 525–528. https://doi.org/10.1080/08039488.2017.1346142
Azuela, Gilbert (2019). The implementation and impact of sensory modulation in Aotearoa New Zealand adult acute mental health services: Two organisational case studies
Bailliard and Whigham’s (2017 cited in Wilson 2020) scoping review of 149 studies on Sensory Processing and mental illness found that interventions targeting sensory processing skills such as sensory rooms may contribute to cognitive gains and improve occupational performance.
Brown, C., Stoffel, V., & Munoz, J. P. (2011). Occupational therapy in mental health: A vision for participation. Philadelphia: F.A. Davis Co. Chapter 22 Catana Brown, Patricia Steffen-Sanchez and Rebecca Nicholson
Champagne,T (2018) Sensory Modulation in Dementia Care: Assessment and Activities for Sensory-enriched Care, Jessica Kingsley Publishers, London, 2018, 168 pp., pbk £15.99, ISBN 13: 9781785927331. - Volume 39 Issue 8
Dorn, Emma, Hitch, Danielle and Stevenson, Christopher 2020, An evaluation of a sensory room within an adult mental health rehabilitation unit, Occupational therapy in mental health, vol. 36, no. 2, pp. 105-118, doi: 10.1080/0164212X.2019.1666770.
Im D. S. (2021). Treatment of Aggression in Adults with Autism Spectrum Disorder: A Review. Harvard review of psychiatry, 29(1), 35–80. https://doi.org/10.1097/HRP.0000000000000282
Henriques-Gomes, L. 10 Nov, 2021 Guardian Australia
MacLennan, K., O’’ Brien, S., and Tavassoli, T (2021) In our Own Words: The Complex Sensory Experiences of Autistic Adults. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-021-05186-3
O’Sullivan, J and Fitzgibbon, C. (2017) Sensory Modulation Resource Manual.
Matson, R., Kriakous, S and Stinson, M (2021) The Experiences of Women with a Diagnosis of Borderline Personality Disorder (BPD) Using Sensory Modulation Approaches in an Inpatient Mental Health Rehabilitation Setting, Occupational Therapy in Mental Health, 37:4, 311-331, DOI: 10.1080/0164212X.2021.1933674
NDIS Quality and Safeguards Commission (2020).Regulated Restrictive Practices Guide. Penrith. Australia: NDIS Quality and Safeguards Commission.
Seckman, Angela ; Paun, Olimpia ; Heipp, Biljana ; Stee, Marie ; Keels‐Lowe, Vonda ; Beel, Frank ; Spoon, Cari ; Fogg, Louis ; Delaney, Kathleen R, Evaluation of the use of a sensory room on an adolescent inpatient unit and its impact on restraint and seclusion prevention Journal of child and adolescent psychiatric nursing, 2017-05, Vol.30 (2), p.90-97
Tavassoli, T., Bellesheim, K., P, M,. Wang, A. T., Halpern, D., Gorenstein, M., Grodberg, D., Kolevzon, A., and Buxbaum, J.D. (2016) Measuring Sensory Reactivity in Autism Specrum Disorder: Application and Simplification of a Clinician-Administered Sensory Observation Scale. Journal of Autism and Developmental Disorders, 46 (1), 287 – 293. Hyyps://doi.org/10.1007/s10803-015-2578-3
Van den Boogert F, Sizoo B, Spaan P, Tolstra S, Bouman YHA, Hoogendijk WJG, Roza SJ. (2021) Sensory Processing and Aggressive Behavior in Adults with Autism Spectrum Disorder. Brain Sci. 14;11(1):95. doi: 10.3390/brainsci11010095. PMID: 33466570; PMCID: PMC7828723.
Verhulst, I., MacLennan, K., Haffey, A., & Tavassoli, T. (2022, January 12). The perceived casual relations between sensory reactivity differences and anxiety symptoms in autistic adults.
Unwin, K. L., Powell, G., & Jones, C. R. (2021). The use of Multi-Sensory Environments with autistic children: Exploring the effect of having control of sensory changes. Autism. https://doi.org/10.1177/13623613211050176
Werkman, M.F., Landsman, J.A., Fokkens, A.S. et al. (2022) The Impact of the Presence of Intellectual Disabilities on Sensory Processing and Behavioral Outcomes Among Individuals with Autism Spectrum Disorders: a Systematic Review. Rev J Autism Dev Disord https://doi.org/10.1007/s40489-022-00301-1
Wilson, Haley, "Mental Health Inpatient Hospitalization: What Nursing Can Learn From "Sensory Rooms."" (2020). Honors Theses. 3315. https://scholarworks.wmich.edu/honors_theses/3315
Wright, L. Bennett, S, Meredith, P (2020) ‘Why didn't you just give them PRN?’: A qualitative study investigating the factors influencing implementation of sensory modulation approaches in inpatient mental health units https://doi-org.ezproxy.library.uq.edu.au/10.1111/inm.12693
Zeanah, C. (2018) Handbook of Infant Mental Health Fourth edition. Chapter 19: Sensory Over-responsivity Timothy W Soto, Vivian Ciaramitaro, Alice Carter.
Zimmermann, D. P. S. (2020). Use of a serenity room for sensory modulation (Order No. 28002838). Available from ProQuest Dissertations & Theses Global. (2420652212). https://www.proquest.com/dissertations-theses/use-serenity-room-sensory-modulation/docview/2420652212/se-2?accountid=14723
Australian National Policies, Reports and Frameworks that contain references to Sensory Modulation, Sensory Items, Sensory Rooms or Sensory Approaches.
NDIS QUALITY & SAFEGUARD COMMISSION (2020) Regulated Restrictive Practices Guide
National Mental Health Commission
National Principals to Support the Goal of Eliminating Mechanical and Physical Restraint in Mental Health Services (Mental Health Commission)
Australian National framework for recovery-oriented mental health services: Guide for practitioners and providers (2013)
State Policies, Reports and Frameworks that contain references to Sensory Modulation, Sensory Items, Sensory Rooms or Sensory Approaches.
Mental Health Act 2016 Chief Psychiatrist Policy Mechanical Restraint, QLD (2020) :
Mental Health Act 2016 Chief Psychiatrist Policy Physical Restraint, QLD (2020) :
Admission of children and adolescents to acute mental health inpatient units – Queensland Health Guideline (2021)
Suicide Prevention Health Taskforce – Phase 1 Action Plan (2017) Qld Health
Mental Health Safety and Quality NSW
Chief Psychiatrist Restraint and Seclusion Standard A standard to reduce and eliminate where possible the use of restraint and seclusion applied under the Mental Health Act 2009 (2021) South Australia:
South Australia Policy: Guideline Restraint and Seclusion in Mental Health Services Policy Guideline
Health framework for reducing restrictive interventions Victoria: Victoria Positive Practice Framework
Attachment and Trauma in People with an Intellectual Disability (2008), Positive Solutions in Practice, Office of the Senior Practitioner.
Mental Health Restraint Policy West Australia(2020) West Australia Prevention and early intervention strategies

A Sensory Lens to Explain Sundowning
Sundowning is a term broadly used to describe a set of behaviours occurring in people with or without dementia, which commonly presents later in the afternoon, evening and late at night. Behaviours include confusion, disorientation, anxiety, agitation, yelling and calling out, aggressive outbursts (verbal and/or physical), pacing and wandering.
While not a formal psychiatric diagnosis, the prevalence of sundowning is well recognised and well documented. Some literature suggests rates of sundowning for elderly persons with cognitive impairment such as dementia are as high as 66%. Sundowning can be very challenging to manage and have a significant impact on the person and their loved ones/carers who are supporting them.
Sundowning is a term broadly used to describe a set of behaviours occurring in people with or without dementia, which commonly presents later in the afternoon, evening and late at night. Behaviours include confusion, disorientation, anxiety, agitation, yelling and calling out, aggressive outbursts (verbal and/or physical), pacing and wandering.
While not a formal psychiatric diagnosis, the prevalence of sundowning is well recognised and well documented. Some literature suggests rates of sundowning for elderly persons with cognitive impairment such as dementia are as high as 66%. Sundowning can be very challenging to manage and have a significant impact on the person and their loved ones/carers who are supporting them.
A number of theories exist regarding the possible reason/s for sundowning, though none have demonstrated a high level of scientific evidence to date. Commonly held beliefs about the prevalence of sundowning in people with dementia include:
· Problems with circadian rhythm (the internal body clock) and difficulty differentiating between dream state during sleep and reality
· Misinterpretation of input (light and shadows) which increases confusion, fear & agitation
· Less stimulation after dark to act as a distraction
· A consequence of mood symptoms or medications wearing off in the afternoons
· Unmet physiological needs – hunger, thirst, pain, over tiredness
Sensory Modulation Brisbane has considered sundowning with a sensory lens and whether these behaviours are in fact a consequence of sensory overload. This could apply to people with dementia, Autism Spectrum Disorder and other conditions.
Sensory overload occurs when a person experiences too much sensory input for their system (too loud, too busy, too bright, too fast or too intense) resulting in increased feelings of distress and overwhelm. Think about a baby who has been too stimulated through the day, they will often become overloaded, upset and are much more difficult to settle in the evening. For a person with dementia, sensory overload will have a similar effect and thus could be a significant factor in the occurrence of sundowning behaviours. Some literature has suggested that agitation could be a behavioural response to sensory overstimulation and wandering may be an attempt at self- regulation.
People with cognitive impairment like dementia often experience sensory overload due to difficulties with:
· understanding their unique sensory needs and preferences
· being able to regulate sensory input throughout the day, for example turning down the volume, changing the temperature, opening or closing the door or window covers or even their choice of meal flavours and textures.
· being able to communicate their sensory needs to others, for example telling others when they feel uncomfortable or in pain or timely requests to change sensory input in their environments
To help manage behaviours related to dementia, non-pharmacological measures including environmental assessment and modifications are recommended. Sensory modulation is therefore an effective means of reducing the prevalence and challenging consequences of sundowning behaviours, by actively managing and addressing the experience of sensory overload. Examples of sensory modulation strategies include:
1. Dialling down sensory input into the afternoon and evening, such as –
· Slowly turning down light levels
· Reducing visual movement and business in the environment, including turning off the TV.
· Reducing sound levels/volume, or use of gentle white noise in background to filter out unwanted sound
· Eliminate unwanted scent with products such as nil odour, or using a familiar scent known to be comforting to the person (be mindful not to diffuse scents in public/common spaces as other people may not prefer/like this smell)
2. Use of individually preferred sensory input at the times sundowning can occur, such as –
· Gentle movement like rocking, stretching or swaying
· Deep pressure like weighted items
· Comforting touch like a warm bath or heat pack, snuggly throw rug, familiar tactile items to explore in hands.
3. Engagement in familiar, calming routines and activities in the afternoon and evenings to increase feelings of comfort and stability and reduce experience of unfamiliar and novel sensory input.
4. Access to a book or digital frame with familiar and soothing pictures of family, friends, pets, places.
References
(2011). Khachiyants, N; Trinkle, D; Son, SY & Kim, KY. Sundown Syndrome in Persons with Dementia: An Update. Psychiatry Investigation, 8:275-287
(2022). Rhodus, E; Hunter, E; Rowles, G. Sensory Processing Abnormalities in Community-Dwelling Older Adults with Cognitive Impairment: A Mixed Methods Study. Gerontology and Geriatric Medicine. 8, 1-11 https://doi.org/10.1177/23337214211068290
Link to Online Training – How to Use Sensory Modulation with Aged Care Residents
Sensory Modulation Resource Manual (2017) J O’ Sullivan and C Fitzgibbon.

Acute Care Team Legend Rachel Woolcock using cooling down sensory modulation options.
Recently I met with one of the most experienced and skilled Mental Health Clinical Nurses in Queensland – Rachel Woolcock. Rachel has over 20 years’ experience with Mental Health including acute care and homeless health. Rachel has undertaken Sensory Modulation Brisbane training and applies Sensory Modulation strategies regularly when working with very distressed or agitated clients. Rachel identifies that one of the most beneficial techniques for this client group has been cooling down with the dive reflex response. In her experience, Rachel has found that it is important to acknowledge that the technique sounds 'unusual' or 'a bit funny' but continues to encourage people to try it, with positive outcomes!
Recently I met with one of the most experienced and skilled Mental Health Clinical Nurses in Queensland – Rachel Woolcock. Rachel has over 20 years experience with Mental Health including acute care and homeless health. Rachel has undertaken Sensory Modulation Brisbane training and applies Sensory Modulation strategies regularly when working with very distressed or agitated clients. Rachel identifies that one of the most beneficial techniques for this client group has been cooling down with the dive reflex response. In her experience, Rachel has found that it is important to acknowledge that the technique sounds 'unusual' or 'a bit funny' but continues to encourage people to try it, with positive outcomes!
Cooling down options include:
· Zip lock bags with cold water,
· Cold slushies
· Cold water in sinks,
· Cold stress balls
· Chill towels
· Cold face washer/face cloth/flannel
· Using ice sprays
· Disposable ice packs
· Cold Shower
· Jumping into a cold pool or ocean
· Cold drink
· Ice bucket challenge
Cold temperature can be useful for several reasons:
· It can cool the body when it is hot (eg when anger flushes the face and hands).
· As a calming strategy when anxious or panicking
· As a calming strategy when angry or feeling destructive or aggression.
· Cool water in conjunction with breath holding can invoke the mammalian dive reflex and reduce the heart rate. (this makes it unsuitable for people with heart conditons or anorexia nervosa without prior medical clearance. If you have a medical condion – ask your Doctor if this is ok for you)
· As an intense sensation, it can be an alternative to self harm.
· The sensory input can feel grounding and reduce dissociation.
· To cease hallucinations (we have had a couple of clients try this and found it is the most useful technique that they have found)
How to use cold water to chill:
· The cold items can be held in the hands, or applied to the face or the whole body. Each person can think about what will work for them and also how much cold that they are comfortable with using.
· Using the icy water on the face can be an intense sensation but can provide a very quick calm down strategy.
· Icy water can be either applied from a bowl or applied to the area under the eyes in a zip lock bag filled with water. The breath is then held. The combination of holding our breath and applying icy water activated the mammalian dive reflex. This reflex has the biological function of decreasing our heart rate to preserve the body and brain if a person falls into the icy water. By decreasing the heart rate and increasing carbon dioxide levels in the blood *by holding our breath) our feelings of calm and grounding increase. This technique is used within Sensory Modulation and also within Dialectical Behaviour Therapy as a distress tolerance skill (TIP skill) .
Further suggestions on Sensory Modulation items are in the Sensory Modulation Resource Manual or in the online course:
Using Sensory Modulation Course
Pre-recorded Videos, slides and downloadable infographics and handouts. IT is 5 hours CPD:
Sensory Modulation Resource Manual
DBT skill training handouts and worksheets Linehan (2014)
Intense Sensations Handout
Image description: young woman with dark hair holding a purple gel mask over her face. She would be doing this to calm herself when distressed.

Factors Influencing Occupational Performance
Occupational Therapists have a lead role working with individuals in the area of occupational performance. Occupational performance refers to how a person engages in meaningful and valued activities in their life and can include self care, daily living skills, community living skills, work, leisure and many more.
An Occupational Therapist who is assisting a person with their occupational performance will identify strengths, barriers, supports, problems and solutions to participating in occupational performance. This process often involves an observation of the person undertaking a or a select number of tasks, as well as completion of checklists and standardised assessments. From here, the OT will then identify possible interventions, with regard to the person (P), the environment (E) and the task/occupation (O), aimed to improve or assist their ability to actively engage in the activity, thus enhancing their occupational performance.

Man cutting lettuce with large gardening shears in kitchen
Occupational Therapists have a lead role working with individuals in the area of occupational performance. Occupational performance refers to how a person engages in meaningful and valued activities in their life and can include self care, daily living skills, community living skills, work, leisure and many more.
An Occupational Therapist who is assisting a person with their occupational performance will identify strengths, barriers, supports, problems and solutions to participating in occupational performance. This process often involves an observation of the person undertaking a or a select number of tasks, as well as completion of checklists and standardised assessments. From here, the OT will then identify possible interventions, with regard to the person (P), the environment (E) and the task/occupation (O), aimed to improve or assist their ability to actively engage in the activity, thus enhancing their occupational performance.
There are a variety of occupational therapy assessments which identify whether a person can or cannot participate in certain tasks, and what level of independence they have to perform such tasks. For example, can the person take a shower independently, what level of assistance might they require?
Other assessments can help to identify the underlying factors contributing to the person being able to complete the task. This information can then be used to work with the individual to problem solve possible solutions to these issues, thus enhancing potential to improve independence, occupational performance and quality of life.
Julie O Sullivan and Carolyn Fitzgibbon at Sensory Modulation Brisbane have developed an observation checklist ‘Factors Influencing Occupational Performance’ which expands on the range of factors to include trauma, sensory preferences, and social and environmental factors.
The Factors Influencing Occupational Performance checklist is available as a (free) pdf to download on the Sensory Modulation Brisbane website.

Sensory Reps: repeating sensory strategies until it becomes a habit
Dazza* was a keen soccer player who had been having difficulties with anger and aggression which had resulted in him being sent off the field. He decided to see a Mental Health OT and they had worked out a plan together which involved using Sensory Modulation. Sensory Modulation is an intervention that uses the senses to change how someone feels. His OT had told him about the benefits of changing his feelings in the moment when he was angry by using cooling water to change the anger response in his body. Dazza had experienced a quick calm down after he poured water over his head and could really see how this could assist him with his anger.
He went to his Saturday night Soccer with his cold water bottles and his plan clear in his head. He was very motivated to reduce his anger as he did not want to be the type of person who hurt other people or made them feel uncomfortable.

Dazza* was a keen soccer player who had been having difficulties with anger and aggression which had resulted in him being sent off the field. He decided to see a Mental Health OT and they had worked out a plan together which involved using Sensory Modulation. Sensory Modulation is an intervention that uses the senses to change how someone feels. His OT had told him about the benefits of changing his feelings in the moment when he was angry by using cooling water to change the anger response in his body. Dazza had experienced a quick calm down after he poured water over his head and could really see how this could assist him with his anger.
He went to his Saturday night Soccer with his cold water bottles and his plan clear in his head. He was very motivated to reduce his anger as he did not want to be the type of person who hurt other people or made them feel uncomfortable.
He jogged out to the field feeling positive that he could change his behaviour. He played well and stayed focused on the ball. But things changed in an instant when the referee made the wrong decision. Dazza lost it, slamming the ball to the ground and clenching his fist menacingly at the referee. He was sent off for the rest of the game.
He went back to his OT feeling disillusioned. Dazza’s OT could see that he was motivated to change, as he had gone to the soccer game prepared and had been positive that the calm down strategy would work. So what went wrong?
Dazza had not practiced his new strategy enough to turn it into a habit. His OT introduced Dazza to the concept of Sensory Reps. Sensory Reps involve repeated use of a sensory strategy in the environment in which it is needed to be use. Dazza was encouraged to go to the soccer field every day, to think of something that made him a little irritable and then to run off the field and pour the cold water over his head. His OT explained the research of Ludvig (2019) which found that 50 repetitions were necessary to consolidate a habit. Dazza was also aware that it was very hard for him to think when he got that angry - which explained why the strategies to change his thinking were not working when he was feeling so angry. Dazza was very committed to Soccer and trained most days to keep his ball skills sharp. He understood the importance of practice and added the Sensory Reps exercise to his daily training. Dazza was very pleased when he next saw his OT, relaying his success in his next game. When he became frustrated, he automatically signalled to come off the field and poured the cold water over his head.
*Dazza is a fictional character
References
Sensory Modulation Resource Manual
Ludvig (2019) Train the Brain to Form Good Habits Through repetition: https://neurosciencenews.com/repetition-habit-training-10652/

Intense Sensations to Manage Muscle Cramps and Dissociation
Sensory Modulation Brisbane often discusses the effectiveness of sensory input as a pain competitor, to more effectively manage pain and improve functioning. For example, using temperature, deep pressure or intense scent. It is understood that the application of sensory input interferes with the transmission of pain signals, thus dialling down the intensity.
Intense Sensations to Manage Muscle Cramps
Sensory Modulation Brisbane often discusses the effectiveness of sensory input as a pain competitor, to more effectively manage pain and improve functioning. For example, using temperature, deep pressure or intense scent. It is understood that the application of sensory input interferes with the transmission of pain signals, thus dialling down the intensity.
In 2017, Dr Bruce Bean (acclaimed Neurobiologist at Harvard) commenced extensive research into muscle cramps, which for some people is an incredibly painful and debilitating experience. Dr Bean was interested in why people experience cramps and more effective ways to manage them.
Many theories exist around why people have muscle cramps, including a lack of electrolytes, dehydration, lack of potassium, increased presence of lactic acid and poor fitness levels/reduced training. However many of these theories lack sufficient evidence and/or had been discredited. He understood this to be true also in part due to personal experience. Some years earlier he and a colleague participated in a deep ocean canoeing trip, and despite both men training extensively prior to the trip and maintaining their fluid & electrolyte levels, both still experienced severe muscle cramps.
Dr Bean hypothesised that muscle cramps are less to do with the muscle itself, and more to do with hyper-excitability of the motor neurons (present in the spinal cord) that control the muscle. This is a likely explanation for other related and debilitating conditions including Restless Legs Syndrome (RLS)
An Old Wives’ Tale Spearheads Research
Prior to Dr Bean’s research, in 2009 Kevin Miller (an Exercise Physiologist from the US) investigated the practice of drinking pickle juice to quickly ease muscle cramps. Mr Miller found that it was a highly effective and fast acting intervention. It was deduced that the speed of response (less than 1 minute) was not indicative of a chemical or metabolic change within the muscle, but rather a ‘neurally mediated reflex’ in the oropharyngeal region which inhibited the firing of alpha motor neurons (Miller, et al, 2009)
Dr Bean’s research built on the findings of Mr Miller. He demonstrated that the acetic acid (active ingredient in pickle juice) stimulated discrete sensory neurons in the mouth, stomach & oesophagus. These neurons were connected to/activated TRP (transient receptor potential) channels. TRP channels feed into multiple neural circuits, such as the Vagus nerve and other areas of the brain including the brainstem, which have a strong influence over spinal cord circuitry. Other neurotransmitters (dopamine, serotonin, acetylcholine etc) are also released in this process, which all have input into the spinal cord.
The changes in these neural pathways serve to dampen down the excitability in the motor neurons innervating the muscles, which reduces the experience of cramping. Sensory neurons in the stomach, mouth and oesophagus also have some direct input into the spinal cord, and so could act as an additional modulator of muscle excitation.
Intense Sensations (Taste) Shown to Reduce Muscle Cramps
A variety of strong sensory inputs (taste) have been shown to help reduce muscle cramping by activating TRP channels, including
· Vinegar flavours (pickle juice, yellow mustard)
· Chili peppers
· Bitter flavours (tonic water)*
· Wasabi
· Horse radish
· Cinnamon
· Ginger
* Quinine (used for treating malaria) has historically been promoted as preventing leg cramps despite the lack of robust evidence. People are now warned against using quinine for cramps or muscle pain, due to it increasing the risk of haemorrhage heart arrythmias. Tonic water contains a minimal amount of quinine, and thus the effect is due to the bitter taste and not the quantity of quinine.
Intense Sensations in Dissociation
Intense Sensations have also been used as a grounding strategy in dissociation and as an alternative to self harm in Dialectical Behaviour Therapy and in Sensory Modulation. We are wondering if intense sensations work due to a similar mechanism proposed in cramps. (Possibly the activation of the neutrally mediated reflex in the oropharyngeal region decreases dissociation?) . If there are any scientists reading this blog please let us clinicians know!
The intense taste sensations in the Sensory Modulation Resource Manual include:
· Lemon
· Strong mint
· Warhead or other sour lollies.
· Mouthwash gargling
· Chilli
· Garlic.
We have now updated the intense sensations worksheet to include:
· Wasabi
· Tonic water
· Pickle juice
The updated worksheet is available for downloading (free) at Sensory-Modulation-Brisbane.com and further information is available in the Sensory Modulation Resoruce Manual and the Using Sensory Modulation course.
Resources:
O’Sullivan, J & Fitzgibbon, C (2018) Sensory Modulation Resource Manual Sensory Modulation: Resource Manual eBook: Julie O' Sullivan, Carolyn Fitzgibbon: Amazon.com.au: Kindle Store
Using Sensory Modulation Online Course https://courserebel.com/coursedetailnew.aspx?courseid=264&page=/health
Chaffey, L (2019) Rewiring Pain: a new way to reclaim your life Rewiring pain: A new way to reclaim your life eBook: Chaffey, Lisa J: Amazon.com.au: Kindle Store
Show 1054: The Scientific Explanation for a Weird Remedy (Ar... | The People's Pharmacy
The first 30 minutes of this podcast has an interview with Dr Bean explaining his research into muscle cramps



Sensory Preferences in the Work Environment (Office)
Working from home/ changes to work locations has been one of the many challenges facing individuals during COVID-19. Some people have absolutely loved this change, while others cannot wait to return to the office environment. Are these differences all to do with personality traits? Or the trend towards open office spaces? Occupational therapists would suggest that it may also reflect our diverse sensory preferences.
Working from home/ changes to work locations have been one of the many challenges facing individuals during COVID-19. Some people have absolutely loved this change, while others cannot wait to return to the office environment. Are these differences all to do with personality traits? Or the trend towards open office spaces? Occupational therapists would suggest that it may also reflect our diverse sensory preferences.
What are Sensory Preferences?
Sensory Preferences are the unique likes and dislikes for different types and intensities of sensations in our day to day life. This can include what we see, hear, smell, taste, touch and our body movement. For example, some people like the feeling of strong muscle exercise, prefer music to be played loudly and enjoy intense flavours in their cooking. Other people may prefer gentle movement, lower noise volumes and predictable, familiar tastes. Most people have a variety of sensory preferences which illustrates just how diverse and unique our sensory systems and thus sensory needs really are.
Opportunities to better understand and accommodate our and other people’s sensory preferences can improve quality of life, enhance our performance in everyday activities (including self-care, work and leisure) and improve our relationships.
Sensory Preferences in the Workplace
Sensory preferences can have a significant impact on our experience of the workplace, with respect to the type of work we are drawn to do, the environments where we work best, and our stress levels in the workplace. We have improved work performance and wellbeing when there is a better match between our sensory preferences, our work duties and activities, and the environment in which we work. Less of a match between these elements can diminish feelings of wellbeing and performance in the workplace. Humans have a tendency to try to create a better match for themselves, which can be problematic when people working together have diverse sensory needs. How many times have we all been witness to or involved in drawn out battles over the office air conditioning controls?
To further illustrate, Afina works in an open plan office, but prefers to sit in the section up the back that is more quiet and less busy. A neat, tidy, clutter free desk helps her to feel more organised, less stressed and work more efficiently through her day. However due to staff changes, Afina’s desk was relocated from the back of the office to right near the main entrance and close to the staff kitchen. She found the increased noise and movement around her unsettling and made it harder to focus. She also felt distracted by the noise of people chatting, preparing their lunch and smells from the kitchen. She is now sitting next to her colleague Tony, whom she gets on well with socially, but Tony tends to move around, gets up & down from his desk frequently and chats a lot with staff who pass by. Tony likes the hustle and bustle of this section of the office and is even known to create noise (humming to radio, whistling) when things are ‘too quiet’! While this sensory input seems to help Tony feel more energised and alert throughout the workday, for Afina this input is too overwhelming and impacts negatively on her stress levels and work performance.
Afina understands that she is not just being picky, that her sensory preferences are part of her unique physiology, and that she can apply strategies to assist her to focus in the workplace.
Strategies to Better Meet Sensory Needs in the Workplace
1. Get to know your own sensory preferences
Are you sensitive to certain noises, temperature or visual movement? Do you find it harder to focus when certain sensory input (unexpected sound, certain smell) is present in the environment? Do you find your energy levels really dip if you stay seated at your desk for too long?
The Sensory Preferences Screen (The Office) helps identify:
Different preferences for sensory input commonly experienced in an office environment
Sensory input that is ‘too much’, not noticed, sought out or avoided. This is based on Winnie Dunn’s Sensory Profiles.
Building awareness of sensory patterns can then help us develop potential strategies and modulation techniques to better accommodate/address our sensory needs within the workplace.
2. Turning up sensory input
For those who need increased levels of sensory input for optimum health and to feel regulated, ways of increasing or dialling up sensory input in the workday might include:
Bright lamp or lighting around desk
Colourful screen saver on computer – change at regular intervals
Listen to music with earphones/buds
Water bottle with cold water to sip
Move body at regular intervals - photocopy or fax items, take lunch break outside
Chew on mints/hot lollies
Fan near desk to increase air flow
Desk can be located near busier/louder office areas
It may also be useful to build in additional activities involving strong sensory input around work hours and during leisure time. Different examples include -
Listening to preferred music on the way home/while cooking dinner
Exercise or intense physical activities/pursuits in spare time
Playing with pet dog
Planning social activities with friends
3. Turning down sensory input
For people who are more sensitive to and register sensory input more easily than others, reducing sensory input in the work environment (turning it down) can be helpful. Examples may include:
Sitting in a quieter/ less busy section of the office
Being closer to natural light sources (ie- a window)
Reduced clutter in the immediate environment and on desk
Turn down telephone volume
Wear headphones with quiet music.
Desk located away from the kitchen or scent diffusers
Use product like Nil-Odor to reduce smells in environment
Take breaks away from office environment/in quieter space if possible
Small pot plant on desk or item that represents something familiar and comforting (photo of partner, picture of favourite nature scene etc)
If you are interested in finding out more on Sensory Approaches, you could
read the Sensory Modulation Resource Manual or attend Sensory Modulation Brisbane Online Training
Resources:
Dunn, W (2014). The Model of Sensory Processing, Sensory Profile 2 (updated)
Lombard, A (2014). Sensory Intelligence: why it matters more than IQ and EQ. Metz Press, South Africa
O’Sullivan, J & Fitzgibbon, C (2018) Sensory Modulation Resource Manual
O’Sullivan, J & Fitzgibbon, C (2020) Sensory Preferences Screen (The Office)

Image Description: Crowded office space. A man sitting in a wheelchair is having a conversation with a co-worker. The office looks like it is busy and distracting and has lots of people talking . This office would be hard for people with sensory sensitivities to sound and visual input.

Weighted Blankets: Need for more evidence but definitely not no evidence
Weighted blankets are a popular Christmas present this year and have also been described by Time Magazine as one of the best inventions of 2018 (Source: Choice Magazine.) Gravity weighted blankets have sold over $18 US million dollars worth of weighted blankets yet many experts say that there is no evidence that they work. .
I must admit I am getting a little tired of ‘experts’ being interviewed who state that there is no evidence for weighed blankets. I wonder if they do a recent google search or if they are going on something that they read years ago when the research trials were just beginning.
It would be more accurate to describe that there is strong evidence in some areas and limited evidence in other areas. In research groups, strong and limited evidence is described according to levels of evidence. This table describes the categories of level of evidence.
Weighted blankets are a popular Christmas present this year and have also been described by Time Magazine as one of the best inventions of 2018 (Source: Choice Magazine.) Gravity weighted blankets have sold over $18 US million dollars worth of weighted blankets yet many experts say that there is no evidence that they work.
I must admit I am getting a little tired of ‘experts’ being interviewed who state that there is no evidence for weighted blankets. I wonder if they do a recent google search or if they are going on something that they read years ago when the research trials were just beginning.
It would be more accurate to describe that there is strong evidence in some areas and limited evidence in other areas. In research groups, strong and limited evidence is described according to levels of evidence. This table describes the categories of levels of evidence.
Level of evidence description (Winona State University Evidence Based Practice Tool kit)
Level I
Evidence from a systematic review or meta-analysis of all relevant RCTs (randomized controlled trial) or evidence-based clinical practice guidelines based on systematic reviews of RCTs or three or more RCTs of good quality that have similar results.
Level II
Evidence obtained from at least one well-designed RCT (e.g. large multi-site RCT).
Level III
Evidence obtained from well-designed controlled trials without randomization (i.e. quasi-experimental
Level IV
Evidence from well-designed case-control or cohort studies
Level V
Evidence from systematic reviews of descriptive and qualitative studies (meta-synthesis).
Level VI
Evidence from a single descriptive or qualitative study
Level VII
Evidence from the opinion of authorities and/or reports of expert committees.
As each research paper is published, the evidence is accumulating that weighted blankets work. In 2020 alone, a quick google scholar search will bring 15 articles up on weighted blankets. This includes a systemic review and randomised control trials. As soon as one systemic review is published it is out of date. For example the 2020 article on systemic review found that there were no randomised control studies for insomnia, but since their search was in 2018, there have been multiple randomised control studies published in this area. It is pretty hard to keep up.
In this blog, I will only refer to Level 1 and Level 2 evidence as this is considered the highest levels of evidence. There are hundreds of research papers for Level 3, 4, 5, 6, 7 levels of evidence.
Level 1: Evidence that a weighted blanket decreases anxiety
A systematic review was conducted on weighted blankets and concluded that ‘ the literature supports the use of weighted blankets for anxiety reduction’
(This article also looked at insomnia however there were less articles available at the time of the review and the ones that I have included here are more recent)
“Credible research suggests that weighted blankets may be an appropriate therapeutic tool. The intervention was reviewed for use in relieving anxiety and it was found to demonstrate some success in reducing anxiety. “
Level 2 Evidence in Insomnia, Adult patients receiving chemotherapy, Adult patients with eating disorders in inpatient setting.
Another systematic review on insomnia is warranted given the recent studies in the last 2 years. This includes:
A randomized controlled study of weighted chain blankets for insomnia in psychiatric disorders
Conclusion:
Weighted chain blankets are an effective and safe intervention for insomnia in patients with major depressive disorder, bipolar disorder, generalized anxiety disorder, or attention deficit hyperactivity disorder, also improving daytime symptoms and levels of activity.
Worth The Weight: Weighted Blanket Improves Sleep And Increases Relaxation. (randomised control trial)
Results:
Objective sleep data from the 28 participants who completed all study requirements showed 7% improvement of Wake After Sleep Onset, 2% decrease in Light Sleep, and slight improvement in Sleep Efficiency (1.5%) and Sleep Maintenance (1.4%) during intervention (all ps < 0.05). Additionally, participants felt they fell asleep faster (13% faster), experienced better sleep quality (14% better), felt more rested in the morning (17% more rested), and felt they slept better through the night without waking up (36% improvement). They also reported feeling 13% less stressed at bedtime and 17% more relaxed while trying to fall asleep.
Conclusion
Using a weighted blanket reduces self-reported feelings of stress, enhances feelings of relaxation, and can improve sleep and reduce time awake at night in people with sleep onset and sleep maintenance issues.
Weighted Blankets: Anxiety Reduction in Adult Patients receiving chemotherapy.
Conclusion: “
This randomised control trial concluded that a standard-weight, medical-grade therapeutic weighted blanket can be safely used to reduce anxiety in patients of various weights, and a visual analog scale can be a reliable indicator of patients' state anxiety.
An RCT that assesses the efficacy of weighted blankets on anxiety for patients with severe anorexia nervosa (AN) and avoidant restrictive food intake disorder (ARFID) in an inpatient medical setting. The results demonstrate clinical significance, advancing the field of OT as it supports the use of a sensory intervention to positively impact psychological and emotional states of a patient population with limited evidence to support best practices.
Low levels but not no evidence that weighted blankets improve sleep in Autistic children.
There has been some research on using weighted blankets with autistic children that have not found strong levels of evidence of the benefits. However, the weighted blanket was favored by children and parents, and blankets were well tolerated over this period in this study. There has also been some research with small number that have shown positive benefits, but these need to be larger scale and randomised to add to the evidence base .
In my opinion, this is a tricky area to research due to the sensory over and under responsivity of Autistic People. For example, one child may really dislike deep pressure (and therefore weighted blankets) whilst another child may find it very calming. Ideally, the sensory preferences of autistic children would be identified as part of the protocol for future research.
The practice guideline: treatment for insomnia and disrupted sleep behaviour in children and adolescents with autism spectrum disorder stated that: Clinicians should counsel that there is currently no evidence to support the routine use of weighted blankets or specialized mattress technology for improving disrupted sleep. If asked about weighted blankets, clinicians should counsel that the trial reported no serious adverse events with blanket use and that blankets could be a reasonable nonpharmacological approach for some individuals.
Special Mention:
One researcher stands out as having published multiple papers on Weighted Blankets and championing the benefits – Tina Champagne. We can thank Tina for all of her groundbreaking work that has contributed to weighted blankets being recognised as evidence based and in such popular use that it is now considered a great Christmas present. This is one of Tina Champagnes articles:
Mullen and Champagne et al (2008) explored the effectiveness of a thirty pound weighted blanket on thirty-two adults. Vital sign metrics showed that using the weighted blanket in a lying down position was safe. Thirty-three percent of participants experienced a lowering of electro-thermal activity, sixty-three percent reported lower anxiety and seventy eight percent preferred the weighted blanket as a calming modality.
Safety
For people with disabilities and medical conditions it is recommended to discuss the option of a weighted blanket with an Occupational Therapist and your treating Doctor. This blog is a general description of the benefits and is not advice specific to the individual.
Further Information
Weighted Blankets are a Sensory Modulation intervention using deep pressure stimulation.
Further information on Sensory Modulation is available from:
O Sullivan, J & Fitzgibbon, C (2018) Sensory Modulation Resource Manual
Champagne, T. (2011) Sensory Modulation & Environment: Essential elements of occupation
Using Sensory Modulation Online Course 5 hours CPD.
References
Rachel Ohene, MOT, OTR/L; Christina Logan, MS, OTR/L; Ashlie Watters, PhD; Figaro Loresto, PhD, RN; Kathryn Eron; Philip Mehler, MD, FACP, FAED (2020) Assessing the Impact of Weighted Blankets on Anxiety for Patients With Eating Disorders in an Inpatient Setting: A Randomized Control Trial Pilot
A randomized controlled study of weighted chain blankets for insomnia in psychiatric disorders
Ekholm B, Spulber S, Adler M. (2020) A randomized controlled study of weighted chain blankets for insomnia in psychiatric disorders. J Clin Sleep Med. 2020;16(9):1567–
Danoff-Burg, Sharon & Rus, Holly M & Martir, L & Raymann, Roy. (2020). 1203 Worth The Weight: Weighted Blanket Improves Sleep And Increases Relaxation. Sleep. 43. A460-A460. 10.1093/sleep/zsaa056.1197
Eron, K, Kohnert, L, Watters, A, Logan, C, WEisner-Rose, M, Mehler, P. (2020) Weighted Blanket Use: A systematic Review American Journal of Occupational Therapy, August 2020, Vol. 74, 7411515404. https://doi.org/10.5014/ajot.2020.74S1-PO5511
P Gringras, D Green, BWright, C Rush, M Sparrowhawk, K Pratt, V Allgar, Naomi Hooke, D Moore, Z Zaiwalla and L Wiggs (2014) Weighted Blankets and Sleep in Autistic Children—A Randomized Controlled Pediatrics August 2014, 134 (2) 298-306; DOI: https://doi.org/10.1542/peds.2013-4285
Choice article: https://www.choice.com.au/health-and-body/conditions/trouble-sleeping/articles/do-weighted-blankets-work
Mullen, B., Champagne, T. Krishnamurty, S. Dickson, D & Gao, R. (2008) Exploring the safety and therapeutic effects of deep pressure stimulation using a weighted blanket. Occupational Therapy in Mental Health, 24, 65 -89
Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology
Ashura Williams Buckley, Deborah Hirtz, Maryam Oskoui, Melissa J. Armstrong, Anshu Batra, Carolyn Bridgemohan, Daniel Coury, Geraldine Dawson, Diane Donley, Robert L. Findling, Thomas Gaughan, David Gloss, Gary Gronseth, Riley Kessler, Shannon Merillat, David Michelson, Judith Owens, Tamara Pringsheim, Linmarie Sikich, Aubyn Stahmer, Audrey Thurm, Roberto Tuchman, Zachary Warren, Amy Wetherby, Max Wiznitzer, Stephen Ashwal First published February 12, 2020, DOI: https://doi.org/10.1212/WNL.0000000000009033
Winona State University Evidence Based Practice Tool kit: https://libguides.winona.edu/c.php?g=11614&p=61584
: This level of effectiveness rating scheme is based on the following: Ackley, B. J., Swan, B. A., Ladwig, G., & Tucker, S. (2008). Evidence-based nursing care guidelines: Medical-surgical interventions. (p. 7). St. Louis, MO: Mosby Elsevier.
https://pediatrics.aappublications.org/content/134/2/298.short

Sensory Triggers Screen- Acute Medical Environment
Sensory Modulation and the Hospital Environment
Hospital admissions can be an extremely overwhelming experience, no matter the reason or duration of the stay. A significant contributing factor to this is the experience of sensory triggers, often at heightened levels and unique to the hospital setting. This overstimulation of the senses is further compounded by the person’s difficulty in modulating the environmental input to suit their individual sensory needs due to illness or injuring, having cognitive or mental health issues, and simply not having the ability to control the environment they are inhabiting.
Hospital admissions can be an extremely overwhelming experience, no matter the reason or duration of the stay. A significant contributing factor to this is the experience of sensory triggers, often at heightened levels and unique to the hospital setting. This overstimulation of the senses is further compounded by the person’s difficulty in modulating the environmental input to suit their individual sensory needs due to illness or injuring, having cognitive or mental health issues, and simply not having the ability to control the environment they are inhabiting.
Examples of sensory triggers unique to hospital settings include:
· Noises – beeping of machines, trolleys, moaning of patients
· Sights – hospital equipment, unfamiliar people, bright lights, unwell patients
· Smells – disinfectant, hospital food, bodily fluids
· Touch - transfers, assistance with self-care, injections, pain
Experiencing sensory triggers can result in increased stress and anxiety levels, feeling unsafe, emotional outbursts and aggressive incidents, which as well as extremely distressing for all involved, impact negatively on health outcomes.
However, research conducted across healthcare settings demonstrates that even small sensory changes to the hospital environment can have a positive impacting on patient stress levels and behaviour, thus creating a safer, more trauma informed and recovery informed environment. These positive outcomes have been shown to benefit both patients and staff.
Yakov et al (2017) found that the practice of dimming lights and reducing noise after 4pm in an acute mental health facility was extremely effective in reducing incidents of aggression and the use of restraint.
Ulrich et al (2018) cites numerous research articles supporting the positive impact of exposure to light reflecting natural rhythms, access to nature (like gardens), views of nature and artwork depicting nature has on stress and aggression levels in hospital settings.
The National Safety and Quality Health Service (NSQHS) Standards (2019) state that sensory modulation helps people manage distressing feelings and regain control without the need for restrictive interventions. Sensory modulation is changing how you feel through using your senses (Fitzgibbon & O’Sullivan, 2018). The standards recommend the following sensory informed environmental strategies to reduce the risk of aggression in a healthcare setting:
Allowing people to move around, preferably with access to outside areas
Reducing stimulus such as bright lights or loud noises
Providing privacy using curtains or side lounges.
In a hospital setting, using a Sensory Triggers Screen that was designed for Acute Medical Environment is a valuable method to:
· Identify a person’s sensory triggers and early signs of distress when in hospital
· Gather information regarding a person’s unique sensory needs
· Recommend and implement simple, practical, sensory informed strategies to better meet these sensory needs and where possible alleviate unnecessary stress to improve their hospital stay and recovery
Information to inform the Sensory Triggers Screen -( Acute Medical Environment) can be gathered from a variety of sources, including the patient, carers/significant others and care specialists who know the patient.
Resources:
Copy of infographic: Sensory Modulation Brisbane infographic:
Copy of Screen: Sensory Triggers Screen - Acute Medical Environment
Book: Sensory Modulation Resource Manual
Online Course: Using Sensory Modulation

References:
Australian Care Standards Quality Health Commission (2019). The National Safety and Quality Health Service (NSQHS) Standards, Minimising Patient Harm, Action 5.33, found in https://www.safetyandquality.gov.au/standards/nsqhs-standards/comprehensive-care-standard/minimising-patient-harm/action-533
O’Sullivan J and Fitzgibbon C (2018) Sensory Modulation: Resource Manual. Amazon Digital Services.
Ulrich, R. et al (2018) Psychiatric ward design can reduce aggressive behaviour, Journal of Environmental Psychology, 57:53-66 https://doi.org/10.1016/j.jenvp.2018.05.002
Yakov, S. et al (2017) Sensory Reduction on the General Milieu of a High-Acuity Inpatient Psychiatric Unit to Prevent Use of Physical Restraints: A Successful Open Quality Improvement Trial, Journal of the American Psychiatric Nurses Association DOI: 10.1177/1078390317736136

Bring back the paper bag for Panic involving hyperventilation
I have been reading about using paper bags for hyperventilation that is occurring for panic. An article written by M Tavel and published in an internal medicine journal (2017 ) has recommended paper bags or breath-holding. There is no mention of any of the other breathing techniques that are commonly used in mental health practice.
I have been reading about using paper bags for hyperventilation that is occurring for panic. An article written by M Tavel and published in an internal medicine journal (2017 ) has recommended paper bags or breath-holding. There is no mention of any of the other breathing techniques that are commonly used in mental health practice.
" Once recognized, prevention and control of at least this part of the disorder are usually successful through explanation of symptom causation and how the symptoms can be aborted by either breath-holding or rebreathing into a paper bag. Before one recommends paper bag rebreathing, however, diagnosis of hyperventilation syndrome must be secure, for adverse events may occur if one overlooks serious underlying conditions of acute Myocardial Infarction (MI), pneumothorax, pulmonary embolism, and others".
It is understandable that Paramedics stopped using paperbags whilst in an emergency situation and until the diagnosis of hyperventilation in panic was established. But when the diagnosis has been clearly established, it is unclear to me as to why paperbags have become so unfashionable in mental health practice in Australia? Does anyone else use them? At Sensory Modulation Brisbane , Julie and I find paperbags and other simple sensory techniques are very effective, even for mild hyperventilation.

Teachers: Keeping calm in the classroom
Sometimes it sounds like Mission Impossible to keep calm in a classroom with dozens of noisy kids present. In this blog I will outline some quick strategies using Sensory Modulation in a primary school classroom.
Sensory Modulation is changing how you feel through using your senses.
Take a movement break in the classrrom
Both you and the children in the class can Jump up and down, start jumps, jog on the spot.
Just a couple of minutes of intense exercise can provide a relaxation response through activating the parasympathetic nervous system. This technique has worked for some people for a panic attack. *
Seating
Try sitting on a wedge cushion or wobble stool and use this to make small movements. Sit up, drop your shoulders and take some long breaths out. Push your feet into the floor for grounding.
Icy Water
Icy water held over your eyes can invoke the dive reflex and provide calming. Can you take a quick trip to the bathroom and use this technique there? Have a zip lock bag ready, fill it one third with icy water and hold your breath. This technique should not be used if you have a heart condition or anorexia nervosa as it changes the heart rate quickly.
Some teachers are using this strategy with the whole class ad keep the ziplock bags in the fridge for students or teachers to use.
Weighted Items
Use several wheat packs or a weighted cushion on your lap (up to 10 per cent of your body weight) This can be a very calming sensation
Low stimulation time
Have a low stimulation and calming time for the entire class. Dim the lights, put on some white noise or calming music and use this time to relax and let go of tension.
I hope that you can try these techniques and try one that will work for you. It can be very useful for children to see someone modelling how to stay calm. So if you have a technique that you can try, talk to the kids about t it and see if they would like to try it to.
If you would like to learn more about these techniques, you could purchase the “Sensory Modulation Resource Manual’ or attend the Brisbane based “Sensory Modulation for Teacher Self Care workshop ‘ in September 2019.

How do you do Sensory Modulation on an Impatient Mental Health Unit without a Sensory Room?
A Sensory Room is a dedicated room with an array of sensory items and strategies for people to trial and use to support their development of self-management skills and to change their moods through Sensory Modulation*. Sensory rooms have been found to be useful in many mental health units by those who use them. (Champagne, 2011).
Often people express that they would like to use Sensory Modulation, but that their organisation is unable to fund a Sensory Room or find the space to put one. The good news is that is possible to use Sensory Modulation on an inpatient ward or emergency department without a Sensory Room through the use of low cost or existing sensory items or considering the environment.
A Sensory Room is a dedicated room with an array of sensory items and strategies for people to trial and use to support their development of self-management skills and to change their moods through Sensory Modulation*. Sensory rooms have been found to be useful in many mental health units by those who use them. (Champagne, 2011).
Often people express that they would like to use Sensory Modulation, but that their organisation is unable to fund a Sensory Room or find the space to put one. The good news is that is possible to use Sensory Modulation on an inpatient ward or emergency department without a Sensory Room through the use of low cost or existing sensory items or considering the environment.
Low Cost Sensory Items
Low cost items can be purchased at Discount Department Stores (eg K-Mart) . This can include:
· hand strengtheners
· cushions
· weights
· books
· mints
· herbal teas
· instant ice packs
· stress balls
· earplugs
· scents
· hand creams
The Sensory Modulation Resource Manual has a list of budget sensory items.
Existing Sensory Items
Many inpatient mental health units have items that they could use for Sensory Modulation. This may include:
· Blankets, cushions
· Art or craft equipment
· Music
· Ear plugs
· Lighting – low light, lamps or dimming switches.
· Ice Packs
· Games
A Personal Safety Plan can be useful to introduce to an impatient unit, to identify possible sensory triggers or sensory modulation strategies.
Considering the Environment
Within every environment, whether indoors or outdoors, opportunities exist for sensory modulation or possibly sensory overload. One design solution is to develop a distinct sensory space or zone within the mental health unit. Even within the one room, there can be smaller zones. Spaces can be designed so that people are able to move to the area that suits their unique sensory preferences and needs at the time. Zones may include the following:
· Exercise zone
· Calm garden zone
· Low stimulation zone
· Socialising zone
· Soothing or comfort zone.
Other sensory zone ideas are available in the The Sensory Modulation Resource Manual
In a 2017 study, Yakov et al found that the lowering of lights and sounds on a mental health unit in the late afternoon reduced the rate of seclusion and restraint. Assault rates fell 83 per cent and the need for seclusions fell by 72 per cent.
On August 6th 2019, Sensory Modulation Brisbane is offering a workshop to use Sensory Modulation in Inpatient Mental Health Units. Other workshops are being held on the use of Sensory Modulation for community settings, for people working in the Non Government Agencies, and for Teacher Self Care.
*Sensory Modulation can be defined as ‘changing how you feel through using your senses’. (O’ Sullivan & Fitzgibbon, 2018).
Citations and Resources:
Adams-Leask,K., Varonal, Lisa, Dua., Charu (2018). The benefits of sensory modulation on levels of distress for consumers in a mental health emergency setting. Volume: 26 issue: 5, page(s): 514-519 https://journals.sagepub.com/doi/abs/10.1177/1039856217751988
Champagne, T., (2011) Sensory Modulation & Environment: Essential Elements of Occupation – 3rd edition
https://medicalxpress.com/news/2017-12-noise-psychiatric-icu-calmer-safer.html
S. Forsyth, Angus & Trevarrow, Rebecca. (2018). Sensory strategies in adult mental health: A qualitative exploration of staff perspectives following the introduction of a sensory room on a male adult acute ward. International Journal of Mental Health Nursing. 27. 10.1111/inm.12466.
Hedlund Lindberg, Mathilde & Samuelsson, Mats & Perseius, Kent-Inge & Björkdahl, Anna. (2019). The experiences of patients in using sensory rooms in psychiatric inpatient care. International Journal of Mental Health Nursing. 10.1111/inm.12593.
O’ Sullivan, J., & Fitzgibbon, C (2018) Sensory Modulation Resource Manual.
Svetlana Yakov et al. Sensory Reduction on the General Milieu of a High-Acuity Inpatient Psychiatric Unit to Prevent Use of Physical Restraints: A Successful Open Quality Improvement Trial, Journal of the American Psychiatric Nurses Association (2017). DOI: 10.1177/1078390317736136
Te Pou Mental Health Initiatives: Sensory Modulation: https://www.tepou.co.nz/initiatives/sensory-modulation/103

Using your senses for self-care
Self-care is increasingly identified as a foundation for physical and mental health and wellbeing. It can be explained as self-directed activities a person engages in with the goal of moving towards a more optimal level of health. Self-care activities involve general daily living tasks (such as healthy eating, getting enough sleep and regular exercise) and can incorporate additional self-initiated activities that may be viewed as relaxing (yoga, meditation), pampering (massage, facial, movie) or a social outlet (date night, catching up with friends).
Self-care is increasingly identified as a foundation for physical and mental health and wellbeing. It can be explained as self-directed activities a person engages in with the goal of moving towards a more optimal level of health. Self-care activities involve general daily living tasks (such as healthy eating, getting enough sleep and regular exercise) and can incorporate additional self-initiated activities that may be viewed as relaxing (yoga, meditation), pampering (massage, facial, movie) or a social outlet (date night, catching up with friends).
Self-care is important for everyone, but especially for those who:
· experience heightened levels of stress
· work in helping professions (such as health, welfare and education sectors)
· care for others
Individuals who address their own self-care are better equipped to support other people in meeting their needs. Diminished opportunity or ability to prioritise self-care can contribute to higher levels of burnout and compassion fatigue.
Sensory modulation is the targeted use of sensory input (touch, taste, smell, sight, sound and movement) to change how you feel, and is a fast and highly effective way of addressing self-care. Sensory modulation can turn down stress and anxiety, reduce feelings of anger and overload, or increase feelings of calm, pleasure and safety, by either adding or turning down specific sensory input. In doing this, self-care needs can be better met. Everyone’s preferences are unique, so sensory input must be specific, appropriate, individualised and meaningful. For example, one person may find reclining on the sofa in a quiet corner with a good book the best self-care for them, while others might like to do a work out at the gym or catch up with friends at a bustling restaurant.
Sensory modulation can be used in a variety of ways to promote self-care. If incorporated into daily routines, people can strive for an optimal level of sensory input to help them feel more regulated and in control. At times of distress, sensory input can be used in that moment to reduce stress and turn down intense emotions. Engaging in sensory input/activities with other people can help all parties to self sooth and calm together. This is known as co-regulation and is a very effective way of supporting everyone to develop skills in self-care.
Ways sensory input can be used as part of a person’s daily routine:
· Use your favourite smelling soap or shower gel when showering
· Listen to preferred music while traveling to work or preparing dinner
· Go for a walk during your lunch break to gain movement sensory input
· Have pot plants, flowers or pictures in your home that you enjoy looking at
· Add favourite flavours/herbs/spices into cooking
Ways sensory input can be used in the moment to change feelings:
· Use a cold washer over your eyes and holding your breath to evoke the dive reflex and turn down the stress response.
· Stretch or tense and release muscle groups to provide deep pressure stimulation, to reduce agitation or anxiety and promote calm.
· Chew something with an intense flavour (lemon, mint, spice, chili) to help shift intense feelings in the moment or assist with focus.
· Smell a strong and scent (lavender, eucalyptus, cinnamon) to feel more grounded and connected.
· Squeeze or fidget with something in your hands (stress ball, elastic band) to improve attention and maintain focus.
Ways sensory input can be used to co-regulate and promote ‘collective’ self-care:
· Sensory boxes or spaces in the classroom for students to utilise provides opportunities for self-regulation. Encourage students to create their own sensory kits.
· Classroom sensory ‘moments’ throughout the day to support learning, assist with focus and help with transitions to new learning and tasks.
· Sensory informed activities in aged care or other diversional/ centre based group programs
· Push a child on a swing, or swing next to them, or help them climb a wall, balance on a beam or similar in the playground.
· Reading with a loved one on the sofa with a throw rug on your laps.
For more information on sensory modulation, strategies to promote self-care, co-regulation, sensory kits and sensory diets, see ‘The Sensory Modulation Resource Manual’, available at:
· TES teacher resources at www.tes.com
· bookstores.