using Sensory Modulation as an Intervention: DIN
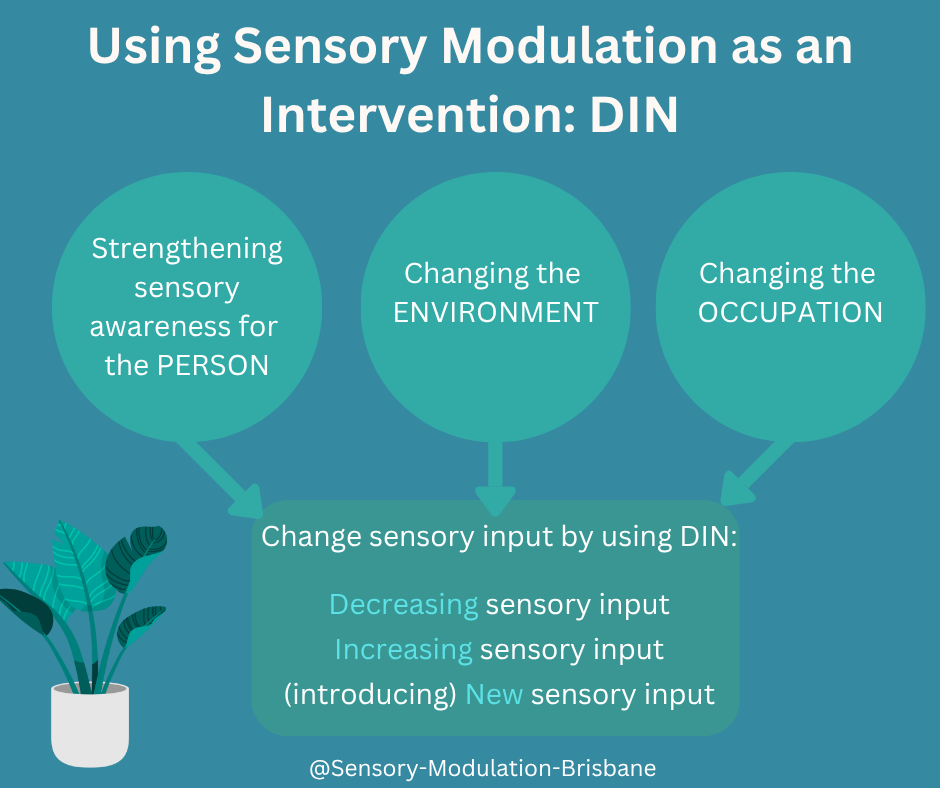
The model proposes that sensory modulation works by addressing the following three constructs:
1. Strengthening sensory awareness for the Person
2. Changing the Environment
3. Changing the Occupation
For each of these three areas, sensory input can be changed by using the acronym DIN -
· Decreasing the sensory input
· Increasing the sensory input
· (introducing) New sensory input

Sensory modulation as an intervention is ‘changing how you feel through using your senses’ (O’Sullivan & Fitzgibbon, 2018). In adjusting specific sensory input, a better match is achieved between the person (and their unique sensory needs), the sensory demands of the environment and their occupations. The person is supported to draw on their strengths, available resources and functional capabilities to enhance participation in meaningful occupations and activities of choice. By honouring an individual’s sensory experiences, and not aiming to mask, or tolerate unique neurology, sensory modulation as an intervention is person-centred, neurodiverse affirming and trauma informed.
Below is a description of the model (shown in the diagram above) using sensory modulation as an intervention. It draws from the PEO Model of occupational performance (Law et al, 1996). The model proposes that sensory modulation works by addressing the following three constructs:
1. Strengthening sensory awareness for the Person
Strengthening awareness of a person’s sensory needs facilitates the development of knowledge, skills and tools regarding unique sensory preferences, capacities, and the environments and activities that best promote functioning. This aligns with the concept of sensory health (Bailliard et al, 2022) and supports the development of agency and expertise.
2. Changing the Environment
This involves:
· The identification and exploration of alternative and beneficial environmental sensory input; or
· Consideration of ways to change sensory aspects of the environment to create a better person-environment fit; or
· Transitioning to a different or preferred environment if more appropriate.
Sensory aspect/s of the environment that do not meet the person’s needs or negatively impact social, emotional and occupational functioning can also be identified and addressed.
3. Changing the Occupation
This involves:
· Exploration of alternative and beneficial sensory input; or
· Consideration of options to adapt/modify aspects of the activity to create a better person-occupation fit; or
· Change the occupation.
Sensory aspect/s of the task not meeting the person’s sensory needs or negatively impacting engagement in preferred occupations and activities can also be identified and addressed.
For each of these three areas, sensory input can be changed by using the acronym DIN -
· Decreasing the sensory input
· Increasing the sensory input
· (introducing) New sensory input
D – Decreasing sensory input
For individuals exhibiting sensory sensitivities, sensory avoidance, trauma histories or neurodivergence, decreasing, avoiding or eliminating certain sensory input can promote safety, autonomy, and participation (Dana, 2018, 2011; Porges, 2011). Reducing sensory input that is unwanted can better align the environment and/or occupations with an individual’s sensory processing needs and occupational goals.
I – Increasing sensory input
Increasing sensory input (intensity, frequency, or predictability) could include moving the body to help with emotion regulation, touch input for grounding and listening to familiar music for calming. Auditory cues to match the demands of the occupation can assist with focus and task engagement. Overstimulation or dysregulation is avoided by ensuring strategies are SAIM (Safe, Appropriate, Individualised and Meaningful) and context relevant. Reducing unwanted or aversive sensory input prior to increasing select sensory input is recommended.
N – (introducing) New sensory input
The new sensory input introduced may be familiar to the person but not usually present in that particular activity or environment. It could be novel to that situation or unfamiliar to the person, such as an unfamiliar food or drink item. New or novel sensory input may be ones that are soothing, grounding or focusing for the person, or ones that help regulate the sensory experience, for example, introducing white noise or nature sounds to help compete with/dial down unwanted sound input or help manage the experience of silence/not enough sound.
Case scenarios to illustrate
Jing’s Sensory Overwhelm in Cooking
Jing experiences sensory overload from olfactory, auditory, and visual stimuli during meal preparation, triggering anxiety, overwhelm and fatigue. Environmental modifications such as using a lid on the saucepan, lowering stove heat, dimming lights, increasing ventilation, and wearing earplugs reduce sensory load, enabling sustained task engagement. Occupational adaptations include breaking the cooking process into smaller tasks completed at different times or delegating components to family members, which supports Jing’s regulation, autonomy, and participation (Edgelow & Cramm, 2020).
Isaac’s sensitivity to Visual Input
Isaac’s trauma history leads to panic and dissociation triggered by bright lighting and visual movement in public spaces. His OT identified strategies such as dimming or redirecting lights, covering fluorescent bulbs, using curtains, or selecting quieter locations to reduce visual stimulation. Occupational modifications include riding as a passenger during heavy traffic and slowing movement pace (e.g., when pushing a wheelchair). Additional self-regulation strategies include wearing a cap or sunglasses and narrowing his visual field. A referral for vision assessment may help address any underlying visual-perceptual contributors to discomfort.
References
Bailliard A, Dunn W, Brown C and Engel-Yeger B (2022) Editorial: Meaningful participation and sensory processing. Front. Psychol. 13:1045650. doi: 10.3389/fpsyg.2022.1045650
Dana, D. A. (2018). The polyvagal theory in therapy: Engaging the rhythm of regulation. W. W. Norton & Company.
Edgelow, M., & Cramm, H. (2020). Developing an Occupation-Centred Framework for Trauma Intervention. Occupational Therapy in Mental Health, 36(3), 270–290. https://doi.org/10.1080/0164212X.2020.1808148
Law M, Cooper B, Strong S, Stewart D, Rigby P, Letts L (1996). The person-environment-occupation model: a transactive approach to occupational performance. Canadian Journal of Occupational Therapy. 63:9–23.
O’Sullivan, J., & Fitzgibbon, C. (2018). Sensory modulation: Changing how you feel through using your senses. Resource Manual. Julie O’Sullivan and Carolyn Fitzgibbon. Brisbanehttp://sensory-modulation-brisbane.com/sensory-modulation-resource-manual.
Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation. W. W. Norton.
The Role of Bubble Columns in Sensory Rooms for Adults: Are They Childlike or Therapeutic?
Sensory rooms are used as spaced for calming and reducing distress in mental health units, schools, nursing homes, shopping centres, sports venues and other community spaces. These rooms are designed to support sensory modulation through calming sensory input such as lighting, textures, sounds, and visual input. One common feature of these rooms, however, raises an important question: the use of bubble columns. These visually appealing, colourful, water-filled tubes are often seen in sensory rooms, but are they still serving their intended purpose, or are they unintentionally reinforcing a sense of infantilisation for adults?
The Role of Bubble Columns in Sensory Rooms for Adults: Are They Childlike or Therapeutic?
Sensory rooms are used as spaced for calming and reducing distress in mental health units, schools, nursing homes, shopping centres, sports venues and other community spaces. These rooms are designed to support sensory modulation through calming sensory input such as lighting, textures, sounds, and visual input. One common feature of these rooms, however, raises an important question: the use of bubble columns. These visually appealing, colourful, water-filled tubes are often seen in sensory rooms, but are they still serving their intended purpose, or are they unintentionally reinforcing a sense of infantilisation for adults?
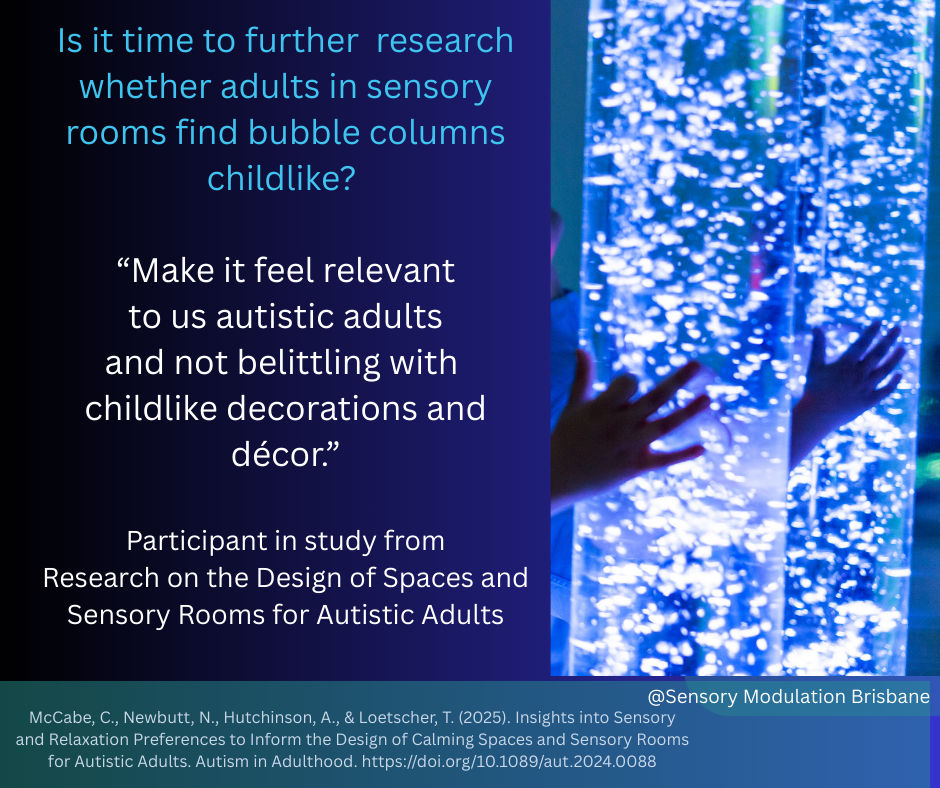
A recent study on the design of sensory spaces for autistic adults shed light on the discomfort some feel when faced with “childlike” décor in spaces that are supposed to offer respite. One participant’s comment stood out: “Make it feel relevant to us autistic adults and not belittling with childlike decorations and décor.” This sentiment points to an issue that has been largely underexplored: Do bubble columns and similar elements unintentionally undermine the autonomy and dignity of adults?
The use of sensory rooms also varies between genders. Studies on psychiatric units have found that females used the sensory room more frequently than males. This pattern has been observed in both adolescent and adult psychiatric populations, where females consistently report higher engagement with sensory interventions compared to males (Novak et al., 2012; McCabe, et al., 2025). While both genders report similar levels of distress reduction following sensory room use, males are often less inclined to engage with these spaces. Novak et al (2012) advised that “Further work is required to ensure that the resources in the sensory room are appropriate for males and that staff are educated about the usefulness of the room for both males and females.” The sensory room features such as bubble columns may be an important resource to research further to identify if it is a factor in some people preferring not to use the sensory rooms.
The Bubble Column: Therapeutic Tool or Overly Infantilising?
Bubble columns have long been used in sensory rooms, primarily due to their calming effect. The slow, mesmerizing rise of bubbles, combined with gentle light displays, can help regulate sensory input, providing a soothing experience for many individuals. These columns are often praised for their ability to offer sensory stimulation in a controlled and predictable manner. However, their design—vibrant, brightly coloured, and somewhat whimsical—tends to evoke a sense of playfulness or even childishness.
For children, this may be fitting. Sensory rooms designed for young individuals frequently incorporate playful, engaging elements meant to spark curiosity and excitement. But when we apply these same designs to environments intended for adults—particularly autistic adults who may already feel marginalized or misunderstood—the question arises: Are we perpetuating a sense of infantilization?
Adults have specific needs and challenges that differ from those of children. They may seek sensory regulation or relief, but the environmental cues that work for them could be vastly different from those that appeal to children. In this context, bubble columns might feel out of place, especially if they evoke memories of childhood experiences or suggest that the space was not truly designed for adult needs.
The Desire for Relevant Design
When the participants in the aforementioned research called for spaces that felt relevant to them as autistic adults, they were asking for an environment that respects their maturity and individuality. We have heard similar comments from other adults that appreciate the sensory rooms for reducing distress and inducing calm but express that some design features do not reflect their adult experiences or needs.
For many individuals, sensory modulation is about finding comfort and relief, not necessarily about engaging with childish décor. Instead of bubble columns, perhaps sensory rooms for adults could be consulted regarding design considerations such as more neutral tones, dimmer lights, minimalistic elements, or even nature-inspired designs that encourage calm without feeling infantilising.
A Call for More Research
Is it time to reconsider the use of bubble columns in sensory rooms for adults? Absolutely. While these columns may offer therapeutic benefits, they should not be the default solution for all sensory spaces. More research is needed to understand the specific preferences of adults when it comes to sensory modulation and room design. This includes exploring whether certain designs, like bubble columns, are seen as infantilising or, conversely, if they truly enhance the sensory experience for adults.
There is also a need for more inclusive design practices that involve autistic adults, sensory room users and adults with mental illness in the conversation about what works for them.
Conclusion
The use of bubble columns in sensory rooms for adults is a topic that warrants deeper consideration. While they are effective for sensory modulation, they need to be designed carefully to meet the needs of adult user. As we continue to develop sensory spaces that are truly inclusive, it's crucial to involve adults in the conversation and ensure that these spaces are designed to meet their unique needs and preferences, free from assumptions or outdated notions of what feels therapeutic.
Ultimately, the goal should be to create sensory rooms that empower and support individuals in a way that feels dignified and relevant to their experiences—not just for children, but for adults too.
References
McCabe, C, Newbutt, N, Hutchinson, A, and Loetscher T. (2025) Insights into Sensory and Relaxation Preferences to Inform the Design of Calming Spaces and Sensory Rooms for Autistic Adults Autism in Adulthood 0 0:0
West, M., Melvin, G., McNamara, F. and Gordon, M. (2017), An evaluation of the use and efficacy of a sensory room within an adolescent psychiatric inpatient unit. Aust Occup Ther J, 64: 253-263. https://doi.org/10.1111/1440-1630.12358
Novak, T., Scanlan, J., McCaul, N., MacDonald, N. & Clarke, T.(2012). Pilot study of a sensory room in an acute psychiatric unit.Australasian Psychiatry, 20, 401–406, doi:10.1177/1039856212459585
Sutton, D., Wilson, M., Van Kessel, K. & Vanderpyl, J. (2013).Optomizing arousal to manage aggression: A pilot study of sen-sory modulation. International Journal of Health Nursing, 22, 500–511, doi:10.1111/inm.12010

Evidence base for sensory modulation in the reduction of restrictive practice for NDIS participants
Evidence base for Sensory Modulation in the reduction of restrictive practices for NDIS participants
We have recorded a presentation and this is available on youtube.
The reference list for this presentation is available here:

Therapy rooms and waiting rooms: designing for sensory needs
At Sensory Modulation Brisbane, we have been advocating for Universal Design in Mental Health Units for Sensory Sensitivities and we would recommend that this is expanded to therapy rooms, waiting rooms and all health care spaces.
Many people who attend Therapy practices have sensory processing patterns that are more sensitive, more avoiding, or more seeking or more missing of sensations than others and this can vary between different senses. This includes:
· Autistics have sensory processing differences recognised as a diagnostic criteria. (DSM5)
· People with PTSD often have reactivity and hypervigilance to certain sensations
· People with schizophrenia often have auditory processing and visual perception challenges.
· ADHDers frequently have sensory processing differences (Schulze 2020)
· A high percentage of people with mental illness have interoceptive difficulties
Therapy room with grey lounge, green cushions, a white blanket and a plant on a small table. We would remove the aromatherapy sticks though!
At Sensory Modulation Brisbane, we have been advocating for Universal Design in Mental Health Units for Sensory Sensitivities and we also recommend this for therapy rooms, waiting rooms and all health care spaces.
Many people who attend Therapy practices have sensory processing patterns that are more sensitive, more avoiding, or more seeking or more missing of sensations than others and this can vary between different senses. This includes:
· Autistics have sensory processing differences recognised as a diagnostic criteria. (DSM5)
· People with PTSD often have reactivity and hypervigilance to certain sensations
· People with schizophrenia often have auditory processing and visual perception challenges.
· ADHDers frequently have sensory processing differences (Schulze 2020)
· A high percentage of people with mental illness have interoceptive difficulties
It can be useful to design for people with sensory sensitivities as it is easier to add sensory input if needed rather than take it away.
Lighting
· Ideally a dimmable light that is set at the preference level of an individual client
· Curtains or Blinds to block out light
· If there is a florescent light, turn it off and use lamps instead.
Sound
· Improving office acoustics can be very beneficial for everyone in terms of privacy and also reducing distractions and sensory sensitivities and overload.
· It is preferable to not use music in a waiting room environment as people who want music can usually access this on their phone.
Scent
· Scents can be a trauma trigger, allergy trigger or lead to sensory sensitivity and overload. So having a low scent therapy room and waiting room can be very important. For this reason, we do not recommend diffusers in public spaces.
· Sometimes it may be necessary to neutralise odours. Try nil odour drops.
Interoception needs
Sometimes therapy is the place where people relax a little and notice that they need to go to the toilet, drink some water or have some snacks. They may not have noticed these interoceptive needs earlier. Close proximity to toilets, water and food can be useful.
Comfortable Seating
There are many people in pain or who have hypermobility and are attending therapy offices. Comfortable seating can make a big difference.
Calming tools
At Sensory Modulation Brisbane, our favourite sensory tools for offices including a weighted cushion, a box of fidgets, icy water or ice packs and invitations to reduce the lighting or turn on or off the pink/brown/white noise machine.
Visual Movement
Ideally design waiting rooms so that there is not a lot of visual movement eg people walking past, traffic etc. Or provide options to be able to not face this visual movement.
Clear Pathways
It is useful for pathways to be clear and obvious and for signage to be clear. It can also be useful to take pictures of landmarks and have this available on website or new starter information .
Personal preferences
It can be useful to invite individuals to use their preferred fidgets, earplugs, sunglasses, back cushion etc so that they are comfortable
Nature
Access to nature can be calming. A plant or a picture of nature can be good additions to an office
Previous blog posts have discussed changing sensory input within a psychiatric hospital:
Training:
https://sensorymodulationbrisbane.ticketspice.com/sensory-modulation-using-a-sensory-lens-with-clients
References:
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Marcel Schulze, Silke Lux, Alexandra Philipsen et al. Sensory Processing in Adult ADHD – A Systematic Review, 10 September 2020, PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-71514/v1]
chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://assets.researchsquare.com/files/rs-71514/v1/d616340b-9b38-4732-b56f-7c249e0632f7.pdf?c=1631855030
Sugiyama, S., et al(2021). The Auditory Steady-State Response: Electrophysiological Index for Sensory Processing Dysfunction in Psychiatric Disorders. Frontiers in psychiatry, 12, 644541.
Sensory Modulation Resource Manual

Using alternatives to torch light monitoring in Mental Health Unit Design
This blog will outline some of the challenges involved in using torch light to observe clients in mental health units at night and also provide some alternative options. Part of routine mental health care on mental health units is regular observations of people while they are sleeping/lying in bed. These routine observations are undertaken due to their perceived benefit in ensuring safety and wellbeing and to reduce the risk of suicide or severe harm. Nursing staff may need to complete observations up to 4 times per hour overnight and torch light is frequently used.

This blog will outline some of the challenges involved in using torch light to observe clients in mental health units at night and also provide some alternative options. Part of routine mental health care on mental health units is regular observations of people while they are sleeping/lying in bed. These routine observations are undertaken due to their perceived benefit in ensuring safety and wellbeing and to reduce the risk of suicide or severe harm. Nursing staff may need to complete observations up to 4 times per hour overnight and torch light is frequently used.
Veale et al (2019) researched the lived experience of these observations and found that these observations interrupted sleep through the torch light, sounds of staff opening and closing bedroom doors and staff talking to each other. People also reported that they found having somebody enter the room in the middle of the night intimidating and unsettling. For many people, this interruption can then make it difficult to return to sleep.
Improving sleep quality on mental health units is important to improve mental health and reduce suicide risk and decrease use of hypnotic medications. (Gardiner 2022) Improving sleep quality has been found to reduce aggressive incidents for psychiatric inpatients residing in secure facilities such as forensic psychiatric hospitals. (Van Veen et al 2020)
Alternatives to torch light that have been discussed have included remote monitoring systems, location trackers and video trackers. The majority of people found the remote monitoring systems acceptable (Veale et al 2019) but the location tracking and video monitoring have been identified as unsuitable due to privacy concerns. (Guardian, 2022)
Sensory Modulation Brisbane has identified the following remote monitoring systems as possible options to replace torch light observations:
At Sensory Modulation Brisbane, we are calling for Universal Design in Mental Health Units for Sensory Sensitivities and this would include replacing torch light observations. The rationale is that so many mental health diagnoses have people with sensory sensitivities. This would also assist Autistics who were on mental health units. People with other sensory processing preferences could also be catered for through adding in personally preferred input from a base of catering for sensory sensitivities.
Sensory Modulation Brisbane also has recorded an online course which includes information on the importance of changing the environment in healthcare settings: tinyurl.com/4yz7hb4k
https://sensorymodulationbrisbane.ticketspice.com/sensory-modulation-using-a-sensory-
lens-with-clients
#Universaldesigninmentalhealthunitssensorysensitivities #sensory #mental health #autistic #mentalhealth_community #schizophrenia #sensoryprocessingawareness #sensoryprocessingsensitivity #psychiatric #occupationaltherapy
More Information:
“This paper argues that intermittent nursing observations of in-patients at night do not reduce the risk of suicide or severe self-harm. Suicides between 23.00 h and 07.00 h are rare, and these overwhelmingly occur under intermittent observations. Such observation is purely a defensive intervention to document that a patient is safe at a particular time, as there is no engagement. For the large majority of in-patients, it has the unintended consequence of causing sleep deprivation. The intervention may cause harm to in-patients by making their disorder worse and increase their risk during the day. If patients are judged to be at immediate risk, then they should be placed on constant observation. If they are not, then optimising sleep is important for treating a psychiatric disorder and they should be placed on general observations.”
Veale D. Against the stream: intermittent nurse observations of in-patients at night serve no purpose and cause sleep deprivation. BJPsych Bull. 2019 Aug;43(4):174-176. doi: 10.1192/bjb.2018.116. Epub 2019 Feb 11. PMID: 30739621; PMCID: PMC6642991
“For psychiatric inpatients residing in secure facilities such as forensic psychiatric hospitals, worse sleep quality and higher insomnia scores significantly relate to aggression, hostility and violent incidents (Kamphuis et al., 2014). Thus, targeting inpatient sleep quality can help to reduce aggressive incidents in these populations, which is paramount to continued successful psychiatric treatment (Van Veen et al., 2020).”
Maaike M. Van Veen, Julie Karsten, Robbert-Jan Verkes & Marike Lancel (2020) Sleep quality is associated with aggression in forensic psychiatric patients, independent of general psychopathology, The Journal of Forensic Psychiatry & Psychology, 31:5, 699-713, DOI: 10.1080/14789949.2020.1785526
“A systematic search of the literature on the environment and nursing observations at night revealed few studies conducted on a psychiatric ward. A meta-analysis identifies the problems of sleep deprivation through noise on medical wards (DuBose & Hadi, 2016). There are also studies identifying that the large majority of psychiatric inpatients experience insomnia without focusing on the determinants”.
(Haynes, Parthasarathy, Kersh, & Bootzin, 2011; Horne, Hay, Watson, & Anderson, 2018; Keeley, 2010; Muller, Olschinski, Kundermann, & Cabanel, 2016). Improving sleep is important because sleep deprivation makes a psychiatric disorder worse (Krystal, 2012) and increases the risk of suicide (Malik et al., 2014).
“Importantly, sleep duration is negatively correlated with subsequent length of time in hospital (Langsrud, Vaaler, Kallestad, & Morken, 2016). The treatment of insomnia has been shown to lessen psychotic experiences (Freeman et al., 2017), mania, (Harvey et al., 2015), depression and anxiety (Ye et al., 2015).”
Veale, D., Sabriha, A., Pagageorgio, A., Gornay, K (2019) The psychiatric ward environment and nursing observations at night: A qualitative study VL - 27 DO - 10.1111/jpm.12583 JO -Journal of Psychiatric and Mental Health Nursing
“Another procedure of which all patients expressed an overall disapproval was the use of light during night observations. They reported being severely disturbed by the use of torches or by bedroom lights being turned on without warning.
“I probably didn’t really go to sleep. They kept coming in every 15 minutes. Sometimes they turn the florescent room lights on in the night, that’s horrible. They would turn the light on until I made some movement or showed I am ok. Sometimes they would use torches as well but better than lights being turned on. (Participant 1)
“Descriptions of night observations were always followed by a reference by the interviewee to the negative impact it had on their emotional state. In some patients, this contributed to a constant state of anxiety and a feeling of being unsettled.”
“The nurses try to use a lower voltage bulb in an attempt not to startle you. But when the room is dark to begin with any light looks so bright. (Participant 6) “
“Startling is when they come in and I see a silhouette, it really frightens me! (Participant 7)”
“At the end of each interview, participants were encouraged to provide their feedback regarding practices that might improve disturbances in night wards. Suggestions in respect to minimizing light disturbances included the use of night-vision glasses or a CCTV camera (only during night-time). Concerning the reduction of noise, suggestions included the following: installing floor coverings, using soft closing doors or applying foam to the doors to soundproof them. Recommendations for safety concerns included the installation of an alarm in the bedroom and for privacy concerns, neon gas windows which could be controlled by both staff members and patients.”
Veale D. Against the stream: intermittent nurse observations of in-patients at night serve no purpose and cause sleep deprivation. BJPsych Bull. 2019 Aug;43(4):174-176. doi: 10.1192/bjb.2018.116. Epub 2019 Feb 11. PMID: 30739621; PMCID: PMC6642991.
Barrera A, Gee C, Wood A, Gibson O, Bayley D, Geddes J. Introducing artificial intelligence in acute psychiatric inpatient care: qualitative study of its use to conduct nursing observations. Evid Based Ment Health. 2020 Feb;23(1):34-38. doi: 10.1136/ebmental-2019-300136. Erratum in: Evid Based Ment Health. 2021 May;24(2): PMID: 32046991; PMCID: PMC7034347.
Poppy May Gardiner, Florence-Emilie Kinnafick, Kieran C. Breen, Alessandra Girardi & Iuliana Hartescu (2022) Behavioural, medical & environmental interventions to improve sleep quality for mental health inpatients in secure settings: a systematic review & meta-analysis, The Journal of Forensic Psychiatry & Psychology, 33:5, 745-779, DOI: 10.1080/14789949.2022.2111320
https://www.tandfonline.com/doi/full/10.1080/14789949.2022.2111320
“NHS trust criticised over system that films mental health patients in their bedroom “ The Guardian, 2022 https://www.theguardian.com/society/2021/dec/13/nhs-trusts-urged-to-ditch-oxevision-system-covert-surveillance-mental-health-patients
https://www.nsw.gov.au/news/trial-of-pulse-monitoring-for-suicide-prevention
Experience of night environment on the ward survey https://onlinelibrary-wiley-com.ezproxy.library.uq.edu.au/doi/full/10.1111/jpm.12583
This survey may be useful to gather data for pre-post intervention changing the torch light
on the wards.
“The categories identified were used to develop a questionnaire to monitor the ward environment and impact of observations at night (Appendix 2). This could be used in a Quality Improvement Project to improve the quality of sleep on a ward. Ideally, the questionnaire would be used in conjunction with a light and decibel metre and measure of sleep quality to obtain more accurate estimations about the ward environment at night.”
Veale, D., Sabriha, A., Pagageorgio, A., Gornay, K (2019) The psychiatric ward environment and nursing observations at night: A qualitative study VL - 27 DO - 10.1111/jpm.12583 JO - Journal of Psychiatric and Mental Health Nursing

Research Ideas
At Sensory Modulation Brisbane, we have clinicians who often identify topics for research, but who are unable to research them due to time or logistical restraints. We are very aware of the need for further research on Sensory Modulation, so we are going to list ideas through blogs when we have them.
Dear Students and researchers.
At Sensory Modulation Brisbane, we have clinicians who often identify topics for research, but who are unable to research them due to time or logistical restraints. We are very aware of the need for further research on Sensory Modulation, so we are going to list ideas through blogs when we have them.
We request that you acknowledge Sensory Modulation Brisbane (Carolyn Fitzgibbon and Julie O’ Sullivan) as inspiration. Also ,we request that you identify Sensory Modulation as an intervention being championed by Occupational Therapists. We would be very interested in hearing if you do proceed with any of our research ideas. Here are our first ideas:
Use of scent of a familiar person/place to decrease anxiety or panic .
Parents of babies and also people with puppies, use the scent of the person to provide calming. In older children and adults, scent could also be utilised with those who do not feel safe.
OT researchers could use this process:
1. Identify a scent that reminds the person of a safe person, place or memory.
2. Identify a way to incorporate this scent into daily occupations.
3. Assess if anxiety is decreased.
Clinical applications include:
Mum sleeps with a hanky and then child with anxiety takes this to school to assist with separation anxiety
Young man has a sprig of rosemary in his backpack as it reminds him of his Grand Dad’s garden.
Young woman smells the deodorant that her Mum uses when she is anxious. (I had one client who ceased having panic attacks when she tried this)
Person feels safe at the beach, so brings a little jar of sand home, and smells this when feeling anxious.
Soothing and Grounding Sensory Modulation Strategies for clients with Severe Anorexia Nervosa
Clients with severe anorexia nervosa are often asked by treating teams to not exercise due to the energy and calories that this takes. However ceasing exercise often takes away a strategy that has been being used to calm and ground. Other strategies for providing vestibular and proprioceptive input could be explored with this clinical population.
Researchers could use this process:
1. Interview a person with Anorexia Nervosa to explore the type of exercise that they enjoyed.
In collaboration with the individual, explore options for sensory modulation that could be meeting a similar sensory need. This may include:
grounding sensations – squeezing a hand grip or theraputty.
soothing – explore other vestibular options eg hammock , chair swing.
feeling in control – tight clothes such as thermals, T-Jackets.
Or sensory modulation could be used to explore soothing options for clients with anorexia nervosa.
Using warmth with clients with Severe Anorexia Nervosa.
Clients with Anorexia Nervosa on inpatient units are often finding it difficult to maintain their core body temperature.
Sensory Modulation strategies could be increased with these clients including using electric blankets, electric hot water bottles, hand warmers, pyjamas heated in dryers etc.
Clients could be interviewed before and after using a heated item, to explore whether this improved their emotional state.
Reference:
"Sensory Modulation Resource Manual" (2018), J O' Sullivan and C Fitzgibbon
Ideas 2:
The above blog generated some interest so we have added some more_
Do medical procedures increase oral hypersensitivity in children?
Some children develop oral hypersensitivity and some then have difficulty with eating foods with textures. Is it possible that the hypersensitivity developed after medical procedures involving anaesthetics, tubing, and needing medication in oral syringes?
Interview parents of children with oral hypersensitivity and also a control group of parents of children without oral sensitivity. Take a sensory history to identify if children were orally hypersensitive from birth (eg more difficulties with breast feeding, bottles etc) and also the rates of medical procedures.
Are children who are super tasters also orally hypersensitive?
Some people are super tasters. Is there a link between taste sensitivity (super tasters) and oral motor sensitivity?
Nail Biting and Sensory Modulation
Nail biting can have a number of identified causes and solutions. Could sensory modulation work as an intervention?
People who nail bite could be interviewed to identify if nail biting provides them with oral input, pain input, or other sensory input. Then alternative strategies for sensory input could be explored. These may be similar eg replacing oral input with another oral input? Or perhaps different sensory input eg do warm sensations, cool sensations, vibration or deep pressure sensations work to provide sensory input and decrease the need for nail biting?
Using the dive reflex prior to an exam to decrease anxiety.
Many students experience anxiety prior to an exam. One option for decreasing the physiological impact of anxiety is to use cool water and breath holding to invoke the dive reflex. (eg cold water in zip lock bags and held over the eyes whilst breath holding).
Fibromyalgia and light and deep touch.
We have had clinical experience with two clients with fibromyalgia who were sensitive to deep touch, and found light touch calming. Does this occur with other people with fibromyalgia?
Cleaning toilets with scent sensitivity.
Some clients with scent sensitivity have difficulty cleaning toilets or other cleaning tasks. What strategies are the most useful for them to be able to complete this task?
Strategies for people who have sensory sensitivities and are in open plan offices
Several clients have had difficulties with misophonia or scent sensitivity or sound sensitivity within an open plan office. Research could be completed to identify the most useful strategies for coping with this.
Intense Sensations and self-harming.
In the Sensory Modulation Resource Manual*, there is a worksheet with additional intense sensations to those traditionally used within DBT. Which of those intense sensations tend to be most useful for those with urges to self-harm?
5 strategies series.
In the Sensory Modulation Resource Manual*, there is a short list of 5 strategies to trial for symptoms including anxiety, agitation, hallucinations, etc. Research could be conducted to trial these in different clinical populations.
Reference:
"Sensory Modulation Resource Manual" (2018), J O' Sullivan and C Fitzgibbon
Sensory Modulation
Sensory Modulation can be used to change how you feel through using your senses. Sometimes Sensory Modulation is described as useful for calming and alerting but it can be used a lot more widely than this. We have made an infographic to show simply what it can be used for:
