
Sex and Intimacy

Blog – Sensory Modulation Interventions to Support Sexual Intimacy
Sexual intimacy, which includes sex, sexual activities and other intimate activities, for many is an important and meaningful occupational role. Participation in sexual intimacy can be influenced and impacted by a range of factors. This blog suggests that using a sensory lens to explore some of these factors in more detail can be beneficial. Furthermore, sensory solutions can go a long way to help support a person’s feelings of safety, enjoyment and engagement in sexual intimacy.
To better understand sexual intimacy with regard to factors that impact sexual response and arousal, it is helpful to understand the Dual-control model of sexual response. This model was developed by Bancroft and Janssen (2007) and proposes –
Desire is not a state that is either ‘present’ or ‘absent’
Sexual response results from excitation (the accelerator) and inhibition (the brake) acting together
The intensity of a person’s sexual response is dependent on how strongly these systems are activated at any given time
While the excitation system seems to receive much of the attention with regard to sexual response and arousal, it is just as important to understand and address the inhibition system. The inhibition system plays a protective role and as such responds to factors that can result in reducing or blocking sexual arousal. This can include stress, fatigue, pain, feelings of fear, disgust or shame, past trauma, or performance worries.
If inhibition levels are high, it can be helpful to consider addressing the inhibitory factors (reducing pressure on the brake) as a means to enhance sexual response, rather than purely focusing on increasing excitatory factors/stimulation (pumping the accelerator).
Sensory modulation interventions are an effective approach to help address both excitatory and inhibitory factors. This may include –
Decreasing, limiting or eliminating certain unwanted or problematic sensory input
Increasing certain sensory input
Introducing new sensory input
Sensory Modulation Brisbane has just released on demand training ‘Sex, Intimacy and Sensory Modulation’.
There are 2 tailored on demand training packages to choose from –
1. A training package designed for anyone who would like to gain a better understanding of and tailored strategies to support their engagement in sexual intimacy.
2. A training package designed for clinicians, support workers and those supporting individuals who would gain benefit from a better understanding of and tailored strategies to support their engagement in sexual intimacy.
While beneficial for everyone, the training content may be especially helpful for those with sensory sensitivities, sensory differences and distinct preferences, neurodivergence, experience of trauma and physical issues including fatigue and pain. It will increase confidence in supporting the application of a range of tailored sensory informed strategies which go beyond traditional calming and alerting models.
The on demand training highlights the valuable role of sensory modulation in supporting a person’s participation in sexual intimacy and incorporates the following content -
Explanation of sensory modulation as an intervention
Dual control model of sexual response, outlining the role of excitation and inhibition mechanisms and factors that impact on these.
Application of practical sensory modulation strategies to support a person’s sexual intimacy, through:
* Building sensory awareness with regard to sexual intimacy
* Using the DIN model - decreasing, increasing and adding (new) sensory input
* Communication strategies to promote safety, self advocacy and comfort
Slides and handouts are provided to assist with learning and application of content.
For more information on the on demand training:
Sensory Modulation for Sex and Intimacy - clinician version
Sensory Modulation for Sex and Intimacy - self directed version
Homeostatic Sensory Reset Hypothesis Worksheet
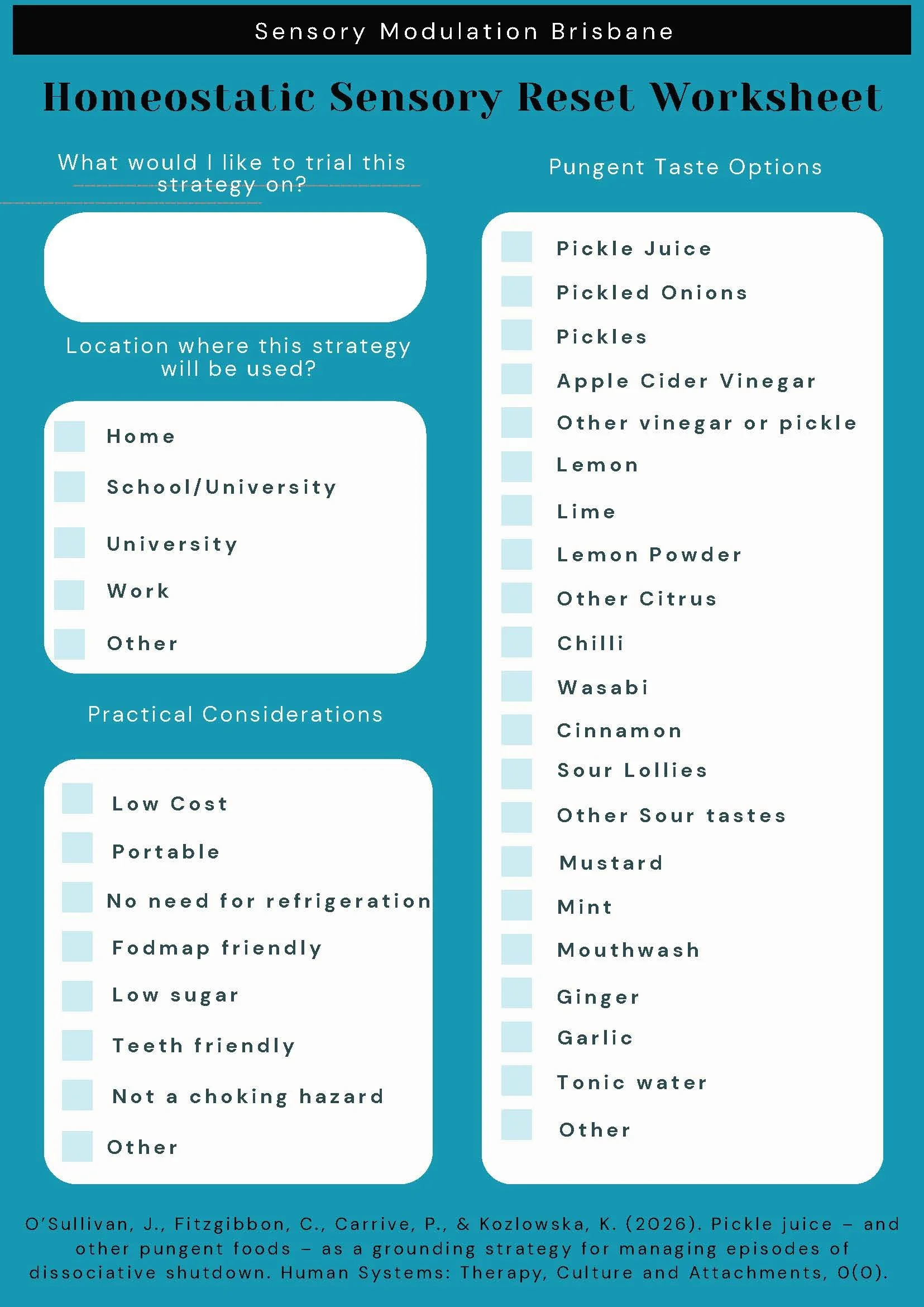
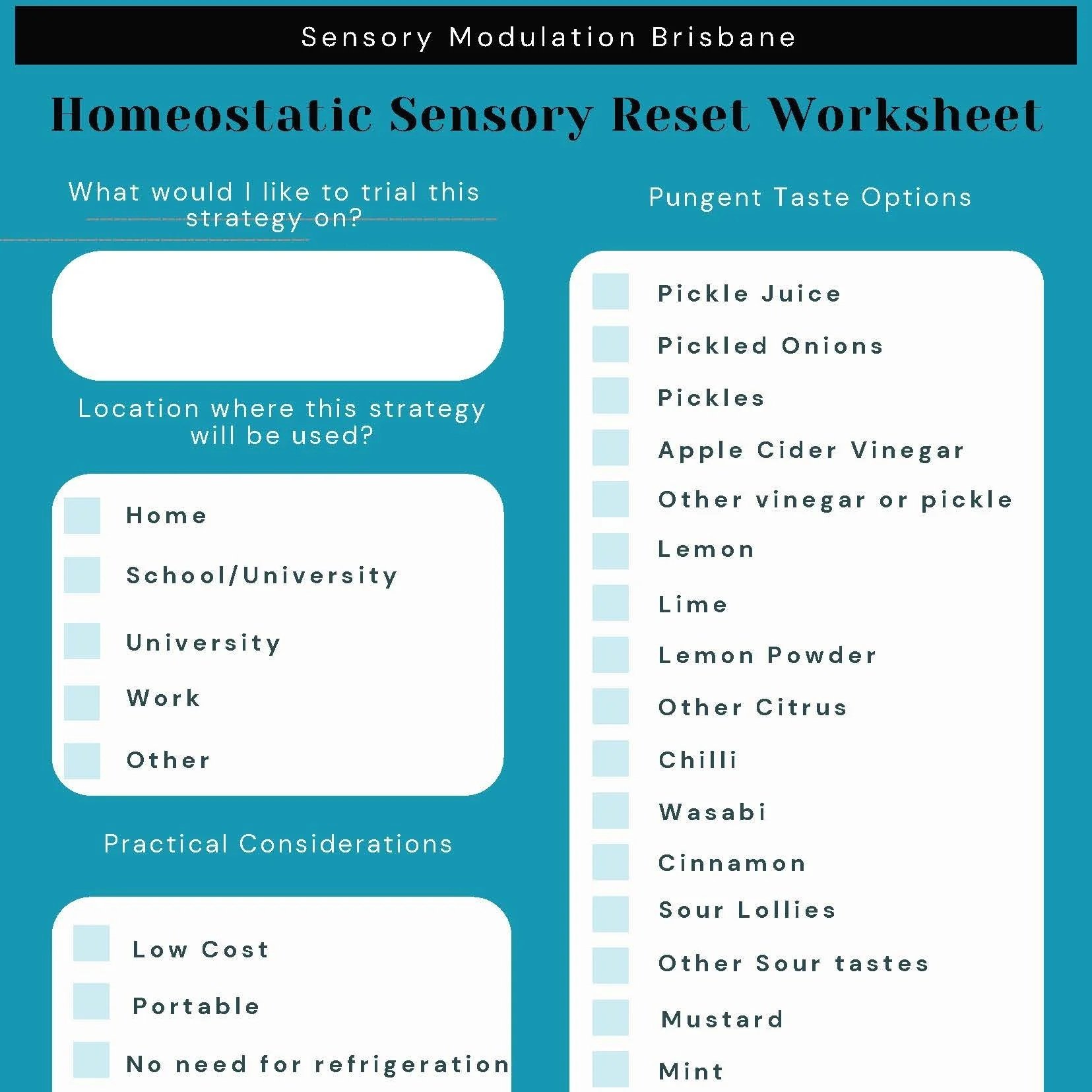
Sensory Modulation Brisbane has developed a worksheet (including a fillable option) to support structured application of the Homeostatic Sensory Reset Hypothesis. The worksheet includes practical considerations to guide safe selection and use of gustatory input within everyday contexts.
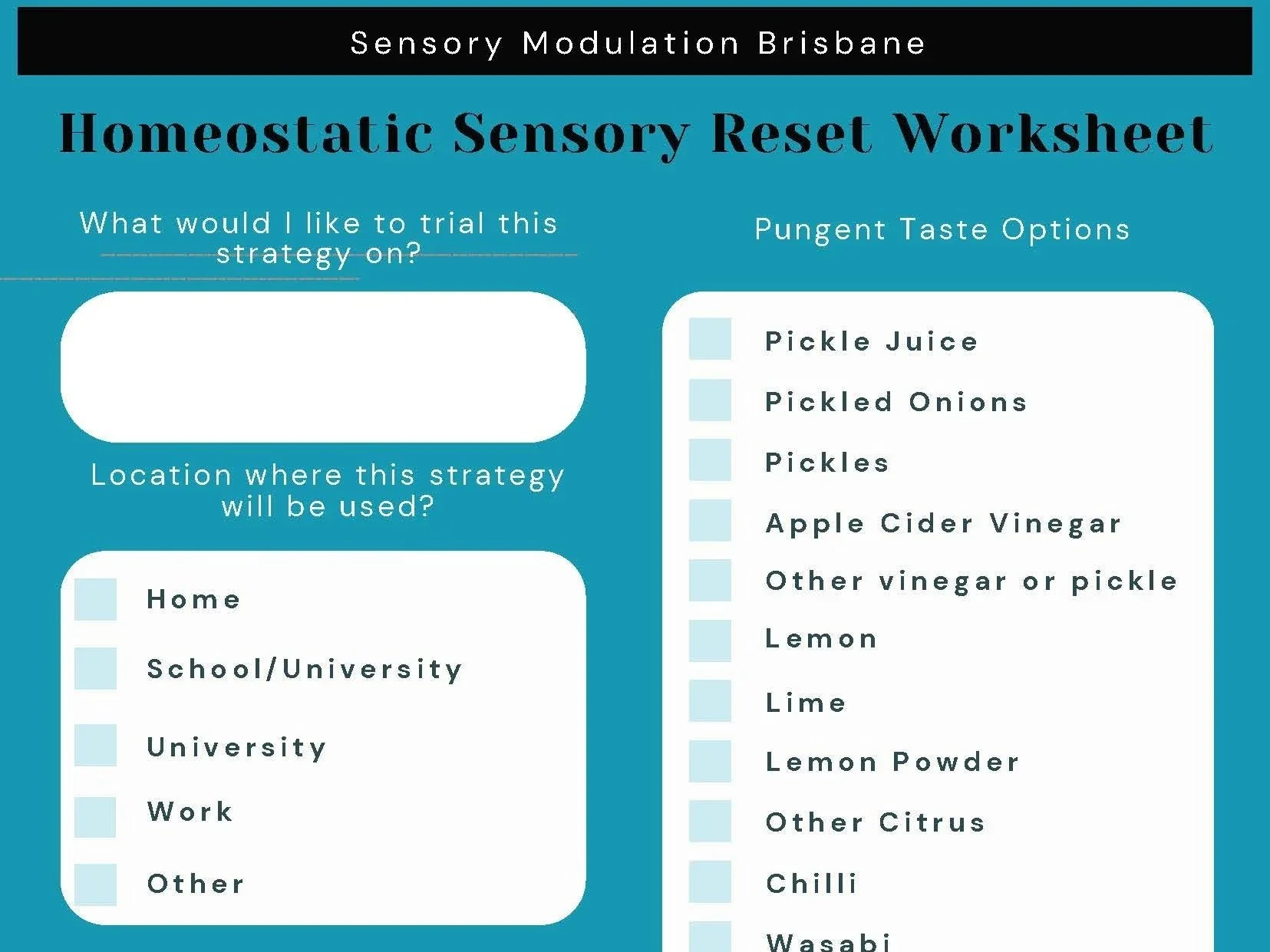
Sensory Modulation Brisbane has developed a worksheet (including a fillable option) to support structured application of the Homeostatic Sensory Reset Hypothesis. The worksheet includes practical considerations to guide the safe selection and use of gustatory input within everyday contexts. The worksheet includes prompts addressing practical considerations, FODMAP requirements, oral care, and intended use of the strategy.
What would I like to trial this strategy for?
Options may include flashbacks, functional seizures, feeling disconnected, dissociated, “spacy”, anger, anxiety, or panic symptoms.
Choosing a pungent taste on a FODMAP diet
People following a FODMAP diet may need to select a pungent taste that aligns with their dietary requirements. Consult a doctor or dietitian for individualised advice.
• Plain pickles (check label for no garlic/onion)
• Apple cider vinegar
• Other plain vinegars (white, rice, malt)
• Lemon/lime/chilli (fresh or dried; small amounts)
• Wasabi (real wasabi powder; check for added garlic)
• Mustard (plain varieties without garlic)
• Mint, ginger
• Tonic water (small serves; check for high fructose corn syrup if from outside Australia)
• Not swallowing is an option
Choosing & considering your teeth
Oral health should be considered, particularly if this strategy is likely to be used regularly. Options selected for frequent use should differ from occasional use.
• Rinse your mouth afterwards
• Consult your dentist for individualised advice
• Consider mouthwash or toothpaste
Generally lower in sugar and less acidic:
• Mint (fresh leaves)
• Ginger (fresh, not candied)
• Mustard (small amounts; non-sugary varieties)
• Wasabi (small amounts)
• Plain pickles occasionally (rinse after)
Choosing & considering flavour intensity
• Disliking a particular flavour is acceptable
• Flavour should be noticeable but not overwhelming, distressing, or associated with negative experiences
• Trial a less intense option if needed
• May be used if sensory sensitive
Practical considerations
Use of any strategy requires consideration of practical factors.
• Where will I need to use it?
• Does it require refrigeration?
• What do I already have available?
• How will I carry it?
Cost
For more information refer to:
O’Sullivan, J., Fitzgibbon, C., Carrive, P., & Kozlowska, K. (2026). Pickle juice – and other pungent foods – as a grounding strategy for managing episodes of dissociative shutdown. Human Systems: Therapy, Culture and Attachments, 0(0). https://doi.org/10.1177/26344041251411521
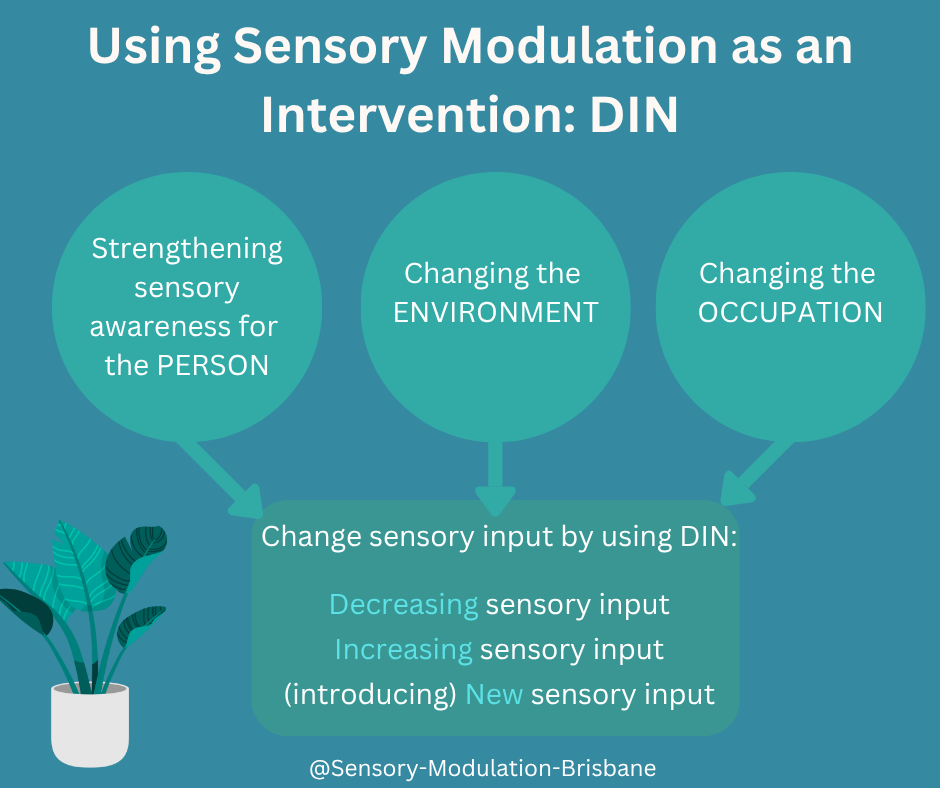
using Sensory Modulation as an Intervention: DIN
The model proposes that sensory modulation works by addressing the following three constructs:
1. Strengthening sensory awareness for the Person
2. Changing the Environment
3. Changing the Occupation
For each of these three areas, sensory input can be changed by using the acronym DIN -
· Decreasing the sensory input
· Increasing the sensory input
· (introducing) New sensory input

Sensory modulation as an intervention is ‘changing how you feel through using your senses’ (O’Sullivan & Fitzgibbon, 2018). In adjusting specific sensory input, a better match is achieved between the person (and their unique sensory needs), the sensory demands of the environment and their occupations. The person is supported to draw on their strengths, available resources and functional capabilities to enhance participation in meaningful occupations and activities of choice. By honouring an individual’s sensory experiences, and not aiming to mask, or tolerate unique neurology, sensory modulation as an intervention is person-centred, neurodiverse affirming and trauma informed.
Below is a description of the model (shown in the diagram above) using sensory modulation as an intervention. It draws from the PEO Model of occupational performance (Law et al, 1996). The model proposes that sensory modulation works by addressing the following three constructs:
1. Strengthening sensory awareness for the Person
Strengthening awareness of a person’s sensory needs facilitates the development of knowledge, skills and tools regarding unique sensory preferences, capacities, and the environments and activities that best promote functioning. This aligns with the concept of sensory health (Bailliard et al, 2022) and supports the development of agency and expertise.
2. Changing the Environment
This involves:
· The identification and exploration of alternative and beneficial environmental sensory input; or
· Consideration of ways to change sensory aspects of the environment to create a better person-environment fit; or
· Transitioning to a different or preferred environment if more appropriate.
Sensory aspect/s of the environment that do not meet the person’s needs or negatively impact social, emotional and occupational functioning can also be identified and addressed.
3. Changing the Occupation
This involves:
· Exploration of alternative and beneficial sensory input; or
· Consideration of options to adapt/modify aspects of the activity to create a better person-occupation fit; or
· Change the occupation.
Sensory aspect/s of the task not meeting the person’s sensory needs or negatively impacting engagement in preferred occupations and activities can also be identified and addressed.
For each of these three areas, sensory input can be changed by using the acronym DIN -
· Decreasing the sensory input
· Increasing the sensory input
· (introducing) New sensory input
D – Decreasing sensory input
For individuals exhibiting sensory sensitivities, sensory avoidance, trauma histories or neurodivergence, decreasing, avoiding or eliminating certain sensory input can promote safety, autonomy, and participation (Dana, 2018, 2011; Porges, 2011). Reducing sensory input that is unwanted can better align the environment and/or occupations with an individual’s sensory processing needs and occupational goals.
I – Increasing sensory input
Increasing sensory input (intensity, frequency, or predictability) could include moving the body to help with emotion regulation, touch input for grounding and listening to familiar music for calming. Auditory cues to match the demands of the occupation can assist with focus and task engagement. Overstimulation or dysregulation is avoided by ensuring strategies are SAIM (Safe, Appropriate, Individualised and Meaningful) and context relevant. Reducing unwanted or aversive sensory input prior to increasing select sensory input is recommended.
N – (introducing) New sensory input
The new sensory input introduced may be familiar to the person but not usually present in that particular activity or environment. It could be novel to that situation or unfamiliar to the person, such as an unfamiliar food or drink item. New or novel sensory input may be ones that are soothing, grounding or focusing for the person, or ones that help regulate the sensory experience, for example, introducing white noise or nature sounds to help compete with/dial down unwanted sound input or help manage the experience of silence/not enough sound.
Case scenarios to illustrate
Jing’s Sensory Overwhelm in Cooking
Jing experiences sensory overload from olfactory, auditory, and visual stimuli during meal preparation, triggering anxiety, overwhelm and fatigue. Environmental modifications such as using a lid on the saucepan, lowering stove heat, dimming lights, increasing ventilation, and wearing earplugs reduce sensory load, enabling sustained task engagement. Occupational adaptations include breaking the cooking process into smaller tasks completed at different times or delegating components to family members, which supports Jing’s regulation, autonomy, and participation (Edgelow & Cramm, 2020).
Isaac’s sensitivity to Visual Input
Isaac’s trauma history leads to panic and dissociation triggered by bright lighting and visual movement in public spaces. His OT identified strategies such as dimming or redirecting lights, covering fluorescent bulbs, using curtains, or selecting quieter locations to reduce visual stimulation. Occupational modifications include riding as a passenger during heavy traffic and slowing movement pace (e.g., when pushing a wheelchair). Additional self-regulation strategies include wearing a cap or sunglasses and narrowing his visual field. A referral for vision assessment may help address any underlying visual-perceptual contributors to discomfort.
References
Bailliard A, Dunn W, Brown C and Engel-Yeger B (2022) Editorial: Meaningful participation and sensory processing. Front. Psychol. 13:1045650. doi: 10.3389/fpsyg.2022.1045650
Dana, D. A. (2018). The polyvagal theory in therapy: Engaging the rhythm of regulation. W. W. Norton & Company.
Edgelow, M., & Cramm, H. (2020). Developing an Occupation-Centred Framework for Trauma Intervention. Occupational Therapy in Mental Health, 36(3), 270–290. https://doi.org/10.1080/0164212X.2020.1808148
Law M, Cooper B, Strong S, Stewart D, Rigby P, Letts L (1996). The person-environment-occupation model: a transactive approach to occupational performance. Canadian Journal of Occupational Therapy. 63:9–23.
O’Sullivan, J., & Fitzgibbon, C. (2018). Sensory modulation: Changing how you feel through using your senses. Resource Manual. Julie O’Sullivan and Carolyn Fitzgibbon. Brisbanehttp://sensory-modulation-brisbane.com/sensory-modulation-resource-manual.
Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation. W. W. Norton.
The Role of Bubble Columns in Sensory Rooms for Adults: Are They Childlike or Therapeutic?
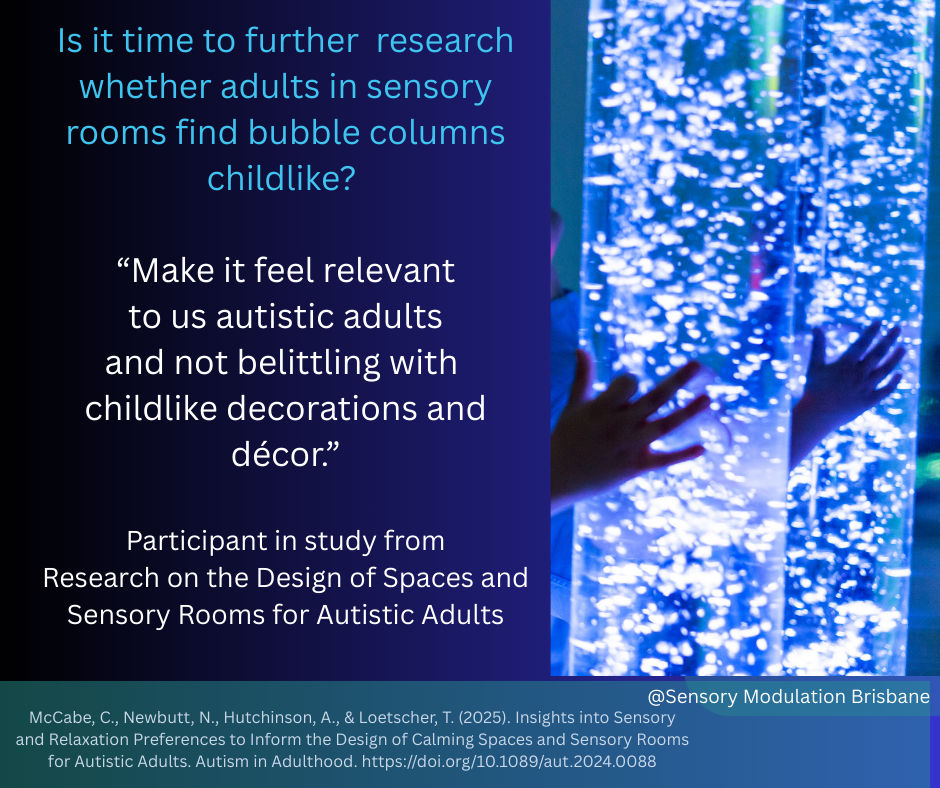
Sensory rooms are used as spaced for calming and reducing distress in mental health units, schools, nursing homes, shopping centres, sports venues and other community spaces. These rooms are designed to support sensory modulation through calming sensory input such as lighting, textures, sounds, and visual input. One common feature of these rooms, however, raises an important question: the use of bubble columns. These visually appealing, colourful, water-filled tubes are often seen in sensory rooms, but are they still serving their intended purpose, or are they unintentionally reinforcing a sense of infantilisation for adults?
The Role of Bubble Columns in Sensory Rooms for Adults: Are They Childlike or Therapeutic?
Sensory rooms are used as spaced for calming and reducing distress in mental health units, schools, nursing homes, shopping centres, sports venues and other community spaces. These rooms are designed to support sensory modulation through calming sensory input such as lighting, textures, sounds, and visual input. One common feature of these rooms, however, raises an important question: the use of bubble columns. These visually appealing, colourful, water-filled tubes are often seen in sensory rooms, but are they still serving their intended purpose, or are they unintentionally reinforcing a sense of infantilisation for adults?
A recent study on the design of sensory spaces for autistic adults shed light on the discomfort some feel when faced with “childlike” décor in spaces that are supposed to offer respite. One participant’s comment stood out: “Make it feel relevant to us autistic adults and not belittling with childlike decorations and décor.” This sentiment points to an issue that has been largely underexplored: Do bubble columns and similar elements unintentionally undermine the autonomy and dignity of adults?
The use of sensory rooms also varies between genders. Studies on psychiatric units have found that females used the sensory room more frequently than males. This pattern has been observed in both adolescent and adult psychiatric populations, where females consistently report higher engagement with sensory interventions compared to males (Novak et al., 2012; McCabe, et al., 2025). While both genders report similar levels of distress reduction following sensory room use, males are often less inclined to engage with these spaces. Novak et al (2012) advised that “Further work is required to ensure that the resources in the sensory room are appropriate for males and that staff are educated about the usefulness of the room for both males and females.” The sensory room features such as bubble columns may be an important resource to research further to identify if it is a factor in some people preferring not to use the sensory rooms.
The Bubble Column: Therapeutic Tool or Overly Infantilising?
Bubble columns have long been used in sensory rooms, primarily due to their calming effect. The slow, mesmerizing rise of bubbles, combined with gentle light displays, can help regulate sensory input, providing a soothing experience for many individuals. These columns are often praised for their ability to offer sensory stimulation in a controlled and predictable manner. However, their design—vibrant, brightly coloured, and somewhat whimsical—tends to evoke a sense of playfulness or even childishness.
For children, this may be fitting. Sensory rooms designed for young individuals frequently incorporate playful, engaging elements meant to spark curiosity and excitement. But when we apply these same designs to environments intended for adults—particularly autistic adults who may already feel marginalized or misunderstood—the question arises: Are we perpetuating a sense of infantilization?
Adults have specific needs and challenges that differ from those of children. They may seek sensory regulation or relief, but the environmental cues that work for them could be vastly different from those that appeal to children. In this context, bubble columns might feel out of place, especially if they evoke memories of childhood experiences or suggest that the space was not truly designed for adult needs.
The Desire for Relevant Design
When the participants in the aforementioned research called for spaces that felt relevant to them as autistic adults, they were asking for an environment that respects their maturity and individuality. We have heard similar comments from other adults that appreciate the sensory rooms for reducing distress and inducing calm but express that some design features do not reflect their adult experiences or needs.
For many individuals, sensory modulation is about finding comfort and relief, not necessarily about engaging with childish décor. Instead of bubble columns, perhaps sensory rooms for adults could be consulted regarding design considerations such as more neutral tones, dimmer lights, minimalistic elements, or even nature-inspired designs that encourage calm without feeling infantilising.
A Call for More Research
Is it time to reconsider the use of bubble columns in sensory rooms for adults? Absolutely. While these columns may offer therapeutic benefits, they should not be the default solution for all sensory spaces. More research is needed to understand the specific preferences of adults when it comes to sensory modulation and room design. This includes exploring whether certain designs, like bubble columns, are seen as infantilising or, conversely, if they truly enhance the sensory experience for adults.
There is also a need for more inclusive design practices that involve autistic adults, sensory room users and adults with mental illness in the conversation about what works for them.
Conclusion
The use of bubble columns in sensory rooms for adults is a topic that warrants deeper consideration. While they are effective for sensory modulation, they need to be designed carefully to meet the needs of adult user. As we continue to develop sensory spaces that are truly inclusive, it's crucial to involve adults in the conversation and ensure that these spaces are designed to meet their unique needs and preferences, free from assumptions or outdated notions of what feels therapeutic.
Ultimately, the goal should be to create sensory rooms that empower and support individuals in a way that feels dignified and relevant to their experiences—not just for children, but for adults too.
References
McCabe, C, Newbutt, N, Hutchinson, A, and Loetscher T. (2025) Insights into Sensory and Relaxation Preferences to Inform the Design of Calming Spaces and Sensory Rooms for Autistic Adults Autism in Adulthood 0 0:0
West, M., Melvin, G., McNamara, F. and Gordon, M. (2017), An evaluation of the use and efficacy of a sensory room within an adolescent psychiatric inpatient unit. Aust Occup Ther J, 64: 253-263. https://doi.org/10.1111/1440-1630.12358
Novak, T., Scanlan, J., McCaul, N., MacDonald, N. & Clarke, T.(2012). Pilot study of a sensory room in an acute psychiatric unit.Australasian Psychiatry, 20, 401–406, doi:10.1177/1039856212459585
Sutton, D., Wilson, M., Van Kessel, K. & Vanderpyl, J. (2013).Optomizing arousal to manage aggression: A pilot study of sen-sory modulation. International Journal of Health Nursing, 22, 500–511, doi:10.1111/inm.12010

Hot Spots and Hot What’s in Sensory Modulation Interventions
Mental Health Units, Emergency Departments and other hospital and care environments are places where higher levels of aggression and frustration can occur. Within these environments there can be specific locations/areas which have an even greater concentration of aggression and frustration. These locations can be described as Hot Spots. (Gillespie et al 2018). In the safe wards literature, the physical environment is one of six domains or categories of factors that can give rise to flashpoints, which have the capacity to trigger conflict and/or containment. (Bowers, 2014).
This article will explore how to identify Hot Spots (and Hot What’s) and some solutions to address them.

Mental Health Units, Emergency Departments and other hospital and care environments are places where higher levels of aggression and frustration can occur. Within these environments there can be specific locations/areas which have an even greater concentration of aggression and frustration. These locations can be described as Hot Spots. (Gillespie et al 2018). In the safe wards literature, the physical environment is one of six domains or categories of factors that can give rise to flashpoints, which have the capacity to trigger conflict and/or containment. (Bowers, 2014).
This article will explore how to identify Hot Spots (and Hot What’s) and some solutions to address them.
To assist with identifying Hot Spots:
1. Listen to lived experience reports and complaints of locations/areas on the units that have negative sensory or other aspects. Eg noisy scraping of chairs in kitchen, loud alarm near nursing station.
2. Use a map of the unit and mark any incidents on the map. Any area that contains a greater frequency of incidents is considered a Hot Spot (Cygnet 2024).
Once the Hot Spots are identified, the next step is to identify the Hot What’s – meaning what sensory or other input is problematic and resulting in the area becoming a Hot Spot.
Hot What’s can be identified by:
1. Listening to lived experience reports and complaints of problematic sensations
2. Completing a sensory audit of the Hot Spot/s, for example identify the sensory input of that place. Using the sensory audit ‘sensory input in mental health units’ might be a good starting point.
3. Completing a sensory audit at the time or not long after the incident. Using the sensory audit tool ‘Sensory Factors in the home environment’ might be helpful.
Solving Hot Spots and Hot What’s:
After identifying the location of the Hot Spots and the Hot What input, it is important to then identify locally achievable solutions. Options to consider include -
1. Change the sensory input (eg replace loud alarms with vibration alarms)
2. Reduce the sensory input for the individual (eg supply sensory modulation items to reduce sensory input such as earplugs, personal scents* to mask other scents. ). Scent needs to be personalised and self applied/not diffused through public spaces. Refer to blog for more information:
3. Support the individual to move away from the input (eg to go outside for a break, offer a different room or a different ward that does not contain the problematic input).
A similar process could be used in a range of different environments including schools, support facilities and housing/accommodation options.
Case Study
An outcome of training conducted by Sensory Modulation Brisbane for Cygnet Health Care in the UK has been greater identification of Hot Spots. The Cygnet OTs were able to identify Hot Spots and then develop sensory modulation plans to change the sensory input or make other changes (eg move the person to another room or space). This process resulted in a significant decrease in seclusion and restraint incidents.
Definition
Hot What’s = Sensory Modulation Brisbane term to describe the sensory input that is present at hot spots.
References
Bowers L. Safewards: a new model of conflict and containment on psychiatric wards. J Psychiatr Ment Health Nurs. 2014 Aug;21(6):499-508. doi: 10.1111/jpm.12129. Epub 2014 Feb 19. PMID: 24548312; PMCID: PMC4237187.
Cygnet 2024. Sensory Modulation Brisbane completed training at Cygnet and an outcome of this training was greater identification of hot spots. The Cygnet OTs identified hot spots and developed sensory modulation plans to change the sensory input or make other changes.
Gillespie A, Reader TW. Patient-Centered Insights: Using Health Care Complaints to Reveal Hot Spots and Blind Spots in Quality and Safety. Milbank Q. 2018 Sep;96(3):530-567. doi: 10.1111/1468-0009.12338. PMID: 30203606; PMCID: PMC6131356.
Safe Wards: https://www.safewards.net/model/technical































Misophonia – more than just dislike of sounds and how OTs can help
Most people can relate to the experience of certain noises or sensations as being really unpleasant. For example, the thought of nails scratching down a blackboard can make the hairs on your arms to stand up, your teeth feel ‘on edge’ and the strong impulse to quickly cover your ears to stop the noise!
The term “misophonia” (hatred of sound) was first used in the early 2000’s to characterise the experience of an extreme emotional and physical response to certain ordinary, often repetitive, day to day sensory input. It is reported to occur in up to 20% of the population and equally in men and women. The input that evokes the most intense responses tends to be human created orofacial noises like breathing, swallowing, chewing, sniffing, throat clearing and lip smacking. Noises such as tapping and pen clicking have also been reported to be problematic. For people with misophonia, these experiences can evoke intense responses that may not seem in keeping with the circumstance such as disgust, irritation, anxiety, distress, anger and an overwhelming desire to remove themselves or remove the input from their environment.
Rather than misophonia being a hearing problem, it is now proposed to stem from attentional or emotional processing issues later in the brain’s auditory system. In examining brain activity while listening to a variety of sounds (including neutral, unpleasant and known misophonia triggers) Kumar et al (2017) found the following:
· the misophonia group rated the trigger sounds as more distressing than the other sounds.
· the research control group rated trigger and unpleasant sounds as similarly annoying.
Most people can relate to the experience of certain noises or sensations as being really unpleasant. For example, the thought of nails scratching down a blackboard can make the hairs on your arms to stand up, your teeth feel ‘on edge’ and the strong impulse to quickly cover your ears to stop the noise!
The term “misophonia” (hatred of sound) was first used in the early 2000’s to characterise the experience of an extreme emotional and physical response to certain ordinary, often repetitive, day to day sensory input. It is reported to occur in up to 20% of the population and equally in men and women. The input that evokes the most intense responses tends to be human created orofacial noises like breathing, swallowing, chewing, sniffing, throat clearing and lip smacking. Noises such as tapping and pen clicking have also been reported to be problematic. For people with misophonia, these experiences can evoke intense responses that may not seem in keeping with the circumstance such as disgust, irritation, anxiety, distress, anger and an overwhelming desire to remove themselves or remove the input from their environment.
Rather than misophonia being a hearing problem, it is now proposed to stem from attentional or emotional processing issues later in the brain’s auditory system. In examining brain activity while listening to a variety of sounds (including neutral, unpleasant and known misophonia triggers) Kumar et al (2017) found the following:
· the misophonia group rated the trigger sounds as more distressing than the other sounds.
· the research control group rated trigger and unpleasant sounds as similarly annoying.
These results support the theory that people with misophonia experience selective intolerance for trigger sounds (Kumar et al, 2017).
When hearing trigger sounds, Kumar also found people with misophonia demonstrate increased insula activation compared to controls, with higher levels of insula activity being correlated with greater reports of distress. The experience of trigger sounds for misophonics showed altered functional connectivity between the insula and other brain regions for attention and emotion. Given the insula plays an important role in internal awareness of body and emotional states, these findings suggest people with misophonia experience altered activation of interoceptive brain networks. Further, it has been proposed that this altered brain connectivity may have similarities to that which occurs in conditions like synesthesia, which is the experience of sensory crossovers (Edelstein et al, 2013)
A study by Kaufman et al (2022) showed people with misophonia have increased sensory responsiveness in the areas of adversive, hedonic, auditory and smell subscales. However they were not identified to have a sensory over-responsiveness type of sensory modulation dysfunction, which suggests that misophonia and SOR, while having some similarities, are actually separate conditions.
The intense adverse response to mouth noises (like chewing) are proposed to be due to heightened sensitivity in the connections between the auditory cortex and orofacial motor control areas. However a research study by Hansen et al (2022) has demonstrated strong connections also between brain regions associated with finger movement & sensation (ie tapping) and the insula.
Further research by Kumar et al in 2021 found that misophonics show increased activity between the auditory cortex and motor control areas related to the face, mouth and throat. Motor regions were not only strongly activated by trigger sounds (not other sounds), but also between visual and motor regions. These findings suggest that discrete visual cues/sensory input can also trigger misophonic responses, possibly due to an involuntary overactivation of the brain’s mirror system resulting in a perception that external trigger sounds are impacting on our bodies without our control.
Samermit et al (2022) investigated whether pairing of different visual stimuli with orofacial sounds (eg a visual of paper tearing paired with the sound of chewing) could alter the misophonic adverse response. Results indicated that this pairing increased the pleasantness of the sound, with the degree of pleasantness further improved if this pairing was presented first. This may indicate that the belief/prior about the sound source might impact on the level of adverse response. Kumar (2021) also suggests that some people can lessen symptom intensity by mimicking the action that generates the trigger sound, possibly by providing the brain with a prediction cue thus reducing novelty and increasing a sense of control.
This research further reflects the complexity of misophonia, including range of triggers and neurological pathways and networks involved, symptoms and functional implications.
The impact of misophonia can be widespread and result in people experiencing many challenges with a range of occupational and functional roles, for example:
· Eating meals with family & in public dining spaces (food courts, restaurants, hospital dining rooms)
· Studying in libraries and open classrooms
· Participating in examination conditions with a group of people
· Shared sleeping arrangements
· Using public transport
· Busy public entertainment venues (cinemas, theatres, concerts)
· Being around others in cold and flu season or being in a health clinic waiting rooms
Continued research and the findings discovered can help us better understand the mechanisms of misophonia and provide clues and recommendations to help in its management.
OTs can offer a range of different tools and strategies to assist people to better understand and manage their unique experience of misophonia, including:
· Education and support to increase people’s understanding and awareness of their experience of misophonia, including –
o specific sensory triggers
o resultant emotional and body responses
o the role that heightened interoceptive (internal body sensory) signals play in misophonia
o the impact of sensory overload on functioning and the importance of energy conservation principles including pacing, taking regular rest breaks, task modification & adaptation to reduce adverse sensory input.
· Sensory modulation strategies to help eliminate or dampen down the experience of the sensory trigger, such as –
o Earplugs such as ear defenders or ear loops
o Modify distance from/ proximity to the trigger (eg – position self further away)
o Adapt the task to alter engagement with the trigger (eg – sit somewhere else or an adjoining room to eat meals, consider a different activity for family connection time like an outdoor walk or board game instead of combined evening meal)
o Strategies to compete with the sensory trigger (use of masking sounds like music, nature sounds or white noise)
o Blue tooth headband for sleep
· Tailored sensory modulation strategies to help reduce stress and manage the emotion dysregulation that can be caused by the experience of misophonia, for example –
o Preferred sensory input
o Sensory routines embedded in day to day activities
· Address/update the brain’s prediction of the sensory input using an intervention combining sensory modulation, predictive processing strategies and sensory health principles
To learn more about Functional Brain Networks for Mental Health:
Sensory Modulation: Using a Sensory Lens with Clients (ticketspice.com)
To learn more about Predictive Processing for Mental Health:
Predictive Processing, Sensory Processing and Mental Health (ticketspice.com)
References
Edelstein M., Brang D., Rouw R., Ramachandran V. S. (2013). Misophonia: physiological investigations and case descriptions. Front. Hum. Neurosci. 7:296. 10.3389/fnhum.2013.00296
Hansen, H., Stefancin,P., Leber, A., Saygin, Z. (2022) Frontiers | Neural evidence for non-orofacial triggers in mild misophonia (frontiersin.org)
Hansen, H. A., Leber, A. B., and Saygin, Z. M. (2021). What sound sources trigger misophonia? Not just chewing and breathing. J. Clin. Psychol. 77, 2609–2625. doi: 10.1002/jclp.23196
Kaufman, A.,Weissman-Fogel. I., Rosenthal, Z., Kaplan Neeman, R., Bar-Shalita, T.(2022). Opening a window into the riddle of misophonia, sensory over-responsiveness, and pain. Frontiers in Neuroscience, https://doi.org//10.3389%2Ffnins.2022.907585
Kumar S, Tansley-Hancock O, Sedley W, Winston JS, Callaghan MF, Allen M, Cope TE, Gander PE, Bamiou DE, Griffiths TD (2017). The Brain Basis for Misophonia. Curr Biol. 2017 Feb 20;27(4):527-533. doi: 10.1016/j.cub.2016.12.048.
Kumar, S., Dheerendra, P., Erfanian, M., Benzaquén, E., Sedley, W., Gander, P., Lad, M., Bamiou, D., Griffiths, T. (2021) The motor basis for misophonia. Journal of Neuroscience. DOI: https://doi.org/10.1523/JNEUROSCI.0261-21.2021
Neurosciencenews.com (2017). The Brain Basis Of "Hatred of Sound": Misophonia - Neuroscience News
Samermit, P., Young, M., Allen, A.K., Trillo, H., Shankar, S., Klein, A., Kay, C., Mahzouni, G., Reddy, V., Hamilton, V., & Davidenko, N. (2022). Development and Evaluation of a Sound- Swapped Video (SSV) Database for Misophonia. Frontiers in Psychology, 13:890829. https://doi.org/10.3389/fpsyg.2022.890829
Samermit, P., Saal, J., & Davidenko, N. (2019). Cross-sensory stimuli modulate reactions to aversive sounds. Multisensory Research, 32(3), 197-213.

Predictive processing, sensory processing and motor control
This blog is part of a series on the implications of predictive processing for clinical practice.
Several people have asked us about praxis and predictive processing and we thought it was useful to write a separate blog on this. We will start by discussing 2 models of sensory processing.
1. Classic detector model of sensory processing. This has been the model for years.
2. Predictive processing model of sensory processing. This is now the leading model of sensory processing in neuroscience literature but is less well known in the clinical area.

Woman with long hair and white dress walking down some steps that look wobbly.
This blog is part of a series on the implications of predictive processing for clinical practice.
Several people have asked us about praxis and predictive processing and we thought it was useful to write a separate blog on this. We will start by discussing 2 models of sensory processing.
1. Classic detector model of sensory processing. This has been the model for years.
2. Predictive processing model of sensory processing. This is now the leading model of sensory processing in neuroscience literature but is less well known in the clinical area.
1.Classic detector model of sensory processing
In the classic detector model, sensory input (bottom up) is detected, processed and integrated to produce actions/motor input. Some sensory input becomes habituated and therefore ‘tuned out’. Some actions are based on the integration of the sensory input and some actions are also automatic (top down). For example to swing a bat, the eyes may register the ball, the position of the arm , integrate this information, make a motor plan that results in action. This can then become automated.
2 Predictive processing model of sensory processing
In the predictive processing model, sensory input is predicted from a top down unconscious model and it is only if sensory input is unexpected that the prediction model is then updated. The unexpected sensory input is known as a prediction error. Despite its name, the term prediction error does not mean that it is wrong or incorrect an error, just that it was not predicted by the prior model. updating the model. A further consideration to note is that the brain may decide to update the model or disregard the input, depending on a few factors that are described as weighting.
In the predictive process model, the brain is trying to minimise prediction errors and to do this , the body can move to make a prediction come true. For example if the brain predicts you will swing a bat at a ball, then the body will do this and then the prediction comes true and remains unaltered. This would occur ‘automatically’ and without conscious awareness. (top down) The only sensory input that would be processed would be unexpected sensory input. So if the swinging the bat at the ball proceeds as predicted, then the sensory input would not need to be registered or processed.
Another example is that if we were walking down stairs, our brain would have a usual ( prior) model of the coordinated body movement and so that would be automatic. If the step was wobbly (and hadn’t been before), this would be unexpected and would be a prediction error. We would have sensory input transmitted to the brain with information on the step, and necessary body movements and the usual (prior) model would be updated.
Interventions
One of the things to keep in mind is that predictive processing is a theory of sensory processing, and that interventions that work, still work, it is just that the theory behind them may be slightly different and there may be a change of emphasis within the interventions.
For Autistic children and by extension other people who also have sensory processing difficulties, there is an increased number of ‘prediction errors’ due to not finding the actions predictable and not generalising the actions. Eg seeing that some actions are more unique than they are. This increases the amount/load of sensory input which can then lead to sensory overload if there is too much of it. It may also be useful to practice body movements in the context that they are being used repetitively so that the brain can learn the prediction.
Further information on predictive processing is available in our course: https://sensorymodulationbrisbane.ticketspice.com/predictive-processing-mental-health-and-sensory-processing

Multisensory top down templates and multi sensory integration
2023 has had a number of articles released on multi sensory integration with some important findings including:
· Multisensory functional brain networks
· Multisensory templates as a top down process
· Multisensory processing occurring at earliest stages of information processing.
Some of the important points from these articles have been included but they are worth reading in their entirety if you are interested in this area.

Multisensory top down templates and multi sensory integration
2023 has had a number of articles released on multi sensory integration with some important findings including:
· Multisensory functional brain networks
· Multisensory templates as a top down process
· Multisensory processing occurring at earliest stages of information processing.
Some of the important points from these articles have been included but they are worth reading in their entirety if you are interested in this area.
Scheliga et al (2023) completed a meta-analysis with multiple sensory modalities to identify a common brain network.
· supports different functional roles for multisensory integration.
· The perception of environmental stimuli mostly occurs on many sites in the nervous system addressing multiple sensory channels at once.
· information in one sense can shape information processing in the other.
· multisensory stimuli evoke a response of the organism that is different from the sum of the unisensory stimuli presented separately.
· the insula may coordinate attention to the information from multiple senses.
· Meanwhile, many studies have shown that MSI takes place at various subcortical levels and that structures like the thalamus integrate different senses even before higher cortical regions are involved
· the insula may coordinate attention to the information from multiple senses.
· Within this network, the thalamus may be the first subcortical relay station projecting multisensory information to a higher cortical integration center, the STG/STS. (STG: superior temporal gyrus, STS: superior temporal sulcus)
Newell et al’s (2023 ) research was on multisensory top–down templates controlling responses in “sensory-specific” cortices and they found that:
“Multisensory objects are selected involuntarily, independently of unisensory task demands,
co-occurring crossmodal stimuli are often easier to:
o detect,
o perceive,
o attend to,
compared with unisensory stimuli, irrespective of the observer's goals
Thus, in multisensory environments, attentional selection is controlled
via integrated top-down object representations, and so not only by
separate sensory-specific top-down feature templates “.
· “To date, processes such as causal inference or predictive coding have mainly been proposed to explain cross-sensory interactions for perception and have not adequately been considered in models of the formation of multisensory object categories in memory, despite the relevance. Given the increasing knowledge of multisensory interactions in the brain, we argue that there is a timely need for an extension of these models. For example, traditionally it was assumed that multisensory integration occurred late in information processing, underpinned by activations in association cortex or beyond in neural structures supporting associative learning and memory. However, evidence for crossmodal interactions in primary sensory regions of the brain, revealing plasticity changes to multisensory inputs at all stages of brain processing, is now overwhelming . Indeed, the past few decades have witnessed growing evidence for multisensory interactions within primary sensory regions of the brain, including activations in the visual cortex to auditory and somatosensory inputs and responses in primary auditory cortex to visual inputs , suggesting that cross-sensory inputs moderate early stages of information processing. “
Choi et al (2023) article describes multiple areas of the brain involved in multi sensory integration. This article is part of a theme issue: ‘Decision and control processes in multisensory perception’.
· prior experience would be one of the major factors that can cause flexible Multisensory integration.
· Therefore, the attention recruited by stimuli in a bottom-up fashion can modulate Multi Sensory Integration, and it is a mechanism that can selectively integrate important and relevant stimuli for the survival of an animal in a complicated environment with numerous sensory inputs.
· Multisensory integration (MSI) occurs in a variety of brain areas, spanning cortical and subcortical regions. In traditional studies on sensory processing, the sensory cortices have been considered for processing sensory information in a modality-specific manner. The sensory cortices, however, send the information to other cortical and subcortical areas, including the higher association cortices and the other sensory cortices, where the multiple modality inputs converge and integrate to generate a meaningful percept. This integration process is neither simple nor fixed because these brain areas interact with each other via complicated circuits, which can be modulated by numerous internal and external conditions. As a result, dynamic MSI makes multisensory decisions flexible and adaptive in behaving animals. Impairments in MSI occur in many psychiatric disorders, which may result in an altered perception of the multisensory stimuli and an abnormal reaction to them. This review discusses the diversity and flexibility of MSI in mammals, including humans, primates and rodents, as well as the brain areas involved. It further explains how such flexibility influences perceptual experiences in behaving animals in both health and disease. This article is part of the theme issue
Sensory Modulation Brisbane has courses available on:
References:
Choi I, Demir I, Oh S, Lee S-H. 2023 Multisensory integration in the mammalian brain: diversity and flexibility in health and disease. Phil. Trans. R. Soc. B 378: 20220338. https://doi.org/10.1098/rstb.2022.0338
Newell, F. N., McKenna, E., Seveso, M. A., Devine, I., Alahmad, F., & Hirst, R. J. (2023). Multisensory perception constrains the formation of object categories: A review of evidence from sensory-driven and predictive processes on categorical decisions. Philosophical Transactions of the Royal Society B: Biological Sciences, 378(1886). https://doi.org/10.1098/rstb.2022.0342
Scheliga, Sebastian, Kellermann, Thilo, Lampert, Angelika, Rolke, Roman, Spehr, Marc and Habel, Ute. "Neural correlates of multisensory integration in the human brain: an ALE meta-analysis" Reviews in the Neurosciences, vol. 34, no. 2, 2023, pp. 223-245. https://doi.org/10.1515/revneuro-2022-0065

Evidence base for sensory modulation in the reduction of restrictive practice for NDIS participants
Evidence base for Sensory Modulation in the reduction of restrictive practices for NDIS participants
We have recorded a presentation and this is available on youtube.
The reference list for this presentation is available here:

Predictive Processing and Body image disturbance in Anorexia Nervosa
When a person with Anorexia Nervosa looks in the mirror, they often report seeing someone who is very overweight rather than the thin body that they actually have.
In the classic detector model of sensory processing, it can be hard to understand how the person can see something that is not reality.
Predictive processing* provides another explanation. that the person is seeing the brains prior model or prediction that they will see, and due to the stress of the condition , they are ‘stuck’ on the predicted model unable to see the reality. A persons predictions are built up from prior experiences and also information from interoception ie feeling fat.

When a person with Anorexia Nervosa looks in the mirror, they often report seeing someone who is very overweight rather than the thin body that they actually have.
In the classic detector model of sensory processing, it can be hard to understand how the person can see something that is not reality.
Predictive processing* provides another explanation. that the person is seeing the brains prior model or prediction that they will see, and due to the stress of the condition , they are ‘stuck’ on the predicted model unable to see the reality. A persons predictions are built up from prior experiences and also information from interoception ie feeling fat.
If you are interested in reading an article, this one is good:
“ Our findings suggest that individuals with AN prioritize interoceptive metacognitive processes (i.e., confidence in their own perceived sensations rather than their actual perceptions), disregarding bottom-up bodily inputs in favour of their prior altered top-down beliefs. Moreover, even if the rehabilitative program partially mitigated these alterations, the pathological condition impaired the patients' ability to coherently update their prior erroneous expectations with real-time multisensory bottom-up bodily information, possibly locking the patients in the experience of a distorted prior top-down belief. These results suggest new therapeutic perspectives and introduce the framework of regenerative virtual therapy (RVT), which aims at utilizing technology-based somatic modification techniques to restructure the maladaptive priors underlying a pathological condition.”
*What is predictive processing:
Predictive Processing is a computational theory of brain functioning where the brain continuously works to minimise error between existing model-based predictions and incoming information (May et al 2021). The theory asserts that the brain generates prior models or predictions of sensory input at multiple levels, generating expectations or inferences regarding future input. This function serves to minimise uncertainties and maximise efficiencies (Wilkinson et al, 2017). Predictive processing as a theory also helps to explain the large number of descending connections in the brain (Walsh et al 2020). In the instances where unpredicted or unexpected sensory input is detected (referred to as a prediction error) this information may pass through these multiple layer and then can update the prior model.
Predictive Processing has been described as “A leading theoretical framework for Sensory Processing” (Tabas et al 2021) and has a lot of ‘explanatory power’ for mental health and sensory processing clinical areas.
Predictive Processing Course:
References:
Di Lernia, D., Serino, S., Tuena, C., Cacciatore, C., Polli, N., & Riva, G. (2023). Mental health meets computational neuroscience: A predictive Bayesian account of the relationship between interoception and multisensory bodily illusions in anorexia nervosa. International Journal of Clinical and Health Psychology, 23(4), 100383. https://doi.org/10.1016/j.ijchp.2023.100383
https://www.sciencedirect.com/science/article/pii/S1697260023000194
Predictive processing: a leading theoretical framework for sensory processing
Predictive Processing is a computational theory of brain functioning where the brain continuously works to minimise error between existing model-based predictions and incoming information (May et al 2021). The theory asserts that the brain generates prior models or predictions of sensory input at multiple levels, generating expectations or inferences regarding future input. This function serves to minimise uncertainties and maximise efficiencies (Wilkinson et al, 2017). Predictive processing as a theory also helps to explain the large number of descending connections in the brain (Walsh et al 2020). In the instances where unpredicted or unexpected sensory input is detected (referred to as a prediction error) this information may pass through these multiple layer and then can update the prior model.
Predictive Processing has been described as “A leading theoretical framework for Sensory Processing” (Tabas et al 2021) and has a lot of ‘explanatory power’ for mental health and sensory processing clinical areas.
When we consider that the brain is largely predicting rather than reacting to sensory input, it may have clinical implications for OTs.

Predictive Processing is a computational theory of brain functioning where the brain continuously works to minimise error between existing model-based predictions and incoming information (May et al 2021). The theory asserts that the brain generates prior models or predictions of sensory input at multiple levels, generating expectations or inferences regarding future input. This function serves to minimise uncertainties and maximise efficiencies (Wilkinson et al, 2017). Predictive processing as a theory also helps to explain the large number of descending connections in the brain (Walsh et al 2020). In the instances where unpredicted or unexpected sensory input is detected (referred to as a prediction error) this information may pass through these multiple layer and then can update the prior model.
Predictive Processing has been described as “A leading theoretical framework for Sensory Processing” (Tabas et al 2021) and has a lot of ‘explanatory power’ for mental health and sensory processing clinical areas.
When we consider that the brain is largely predicting rather than reacting to sensory input, it may have clinical implications for OTs.
OT theories of sensory processing have acknowledged that different people can have different experiences of the same sensory input and the predictive processing theory is a useful explanation for this.
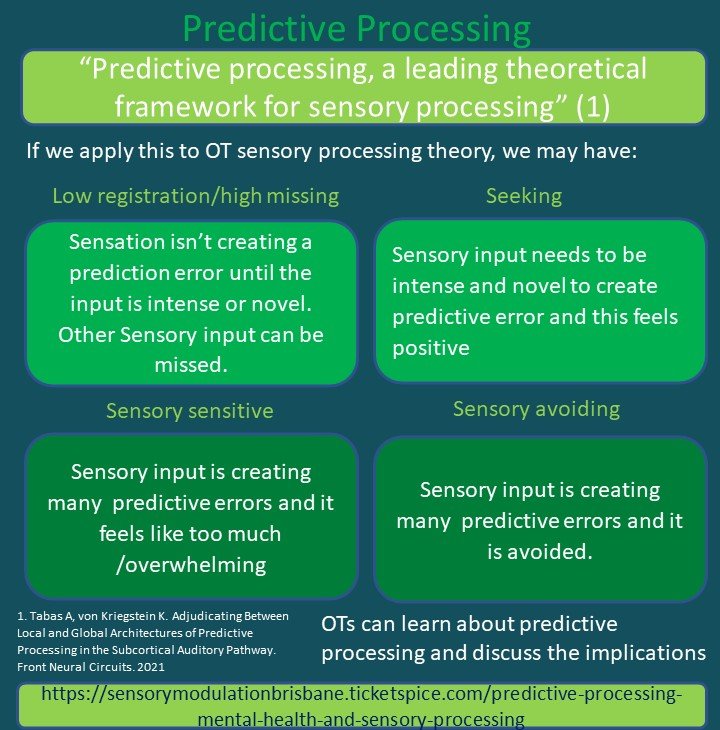
If we apply predictive processing to OT sensory processing theories, we may have:
Low registration/sensory missing
· Sensory input isn’t creating a prediction error until the input is intense or novel. Other sensory input is missed.
Sensory Seeking
· Sensory input needs to be intense and novel to create a predictive error and this feels positive.
Sensory sensitivity
· Sensory input is creating many predictive errors and it feels like too much
Sensory Avoiding
· Sensory input is creating many predictive errors and it is avoided
Julie and Carolyn are clinicians who read widely. We would love to see more discussions in the OT area on predictive processing. We have prepared a training on predictive processing to summarise the information and would hope that OTs can then discuss the clinical implications.
Course on predictive processing
References:
Tabas A, von Kriegstein K. Adjudicating Between Local and Global Architectures of Predictive Processing in the Subcortical Auditory Pathway. Front Neural Circuits. 2021 Mar 12;15:644743. doi: 10.3389/fncir.2021.644743. PMID: 33776657; PMCID: PMC7994860.
“Traditional theories of perceptual processing have failed to adequately explain why sensory cortices are infused with masses of descending connections.
For example, backward projections from V2 to V1 are 10 times more numerous than forward projections from the lateral geniculate nucleus to V1 and the processing of ascending sensory signals is estimated to account for only 1–2% of the brain's energy consumption. “
“Conversely, PP provides a satisfying explanation of these copious backward connections”.
Walsh, K. S., McGovern, D. P., & Clark, A. (2020). Evaluating the neurophysiological evidence for predictive processing as a model of perception. Annals of the New York Academy of Sciences, 1464(1), 242-268. https://doi.org/10.1111/nyas.14321
May, C., Wiitingslow, R. & Blandhol, M (2021). Provoking thought: A predictive processing account of critical thinking and the effects of education, 2458-2468,
Educational Philosophy and Theory
Volume 54, 2022 - Issue 14

Sniff research in Autism
Scent research in Autism
An older article from 2015 on scent and sniffing pleasant and unpleasant odors, noted that Autistics sniffed at pleasant and unpleasant odors with the same intensity whereas neurotypicals sniffed more intensely with pleasant odors and less intensely with unpleasant odors.
We wonder if the more intense sniff is increasing the intensity of the scent and thus contributing to increased sensory overwhelm to scent?
We would love to see some research into whether this could be developed into an easy intervention. We searched articles this week and could not find interventions but please let us know if there are some.
We would propose an intervention where Autistic children could learn to visually identify potentially unpleasant scents (this would need to be individually tailored) and also learn to control the intensity of their sniff to decrease the overwhelm. This could focus on scents that are more commonplace in everyday environments (schools, shops) and where the scent is impacting on occupations.
It has been difficult to research the olfactory (scent) sense in Autism, partly due to the difficulties with accuracy of measurement. A new precise and easy to use system has been developed – the odor pulse ejection system. It is described in this article:
https://www.frontiersin.org/articles/10.3389/fnhum.2020.523456/full
This system was designed to more accurately measure olfactory processing including odor detection, identification and evaluation. Findings of the study using the odor pulse ejection system suggest differences in aspects of olfactory processing for autistics, including olfactory working memory and/or attention.
Xu, M., Minagawa, Y., Kumazaki, H., Okada, K., & Naoi, N. (2020). Prefrontal Responses to Odors in Individuals With Autism Spectrum Disorders: Functional NIRS Measurement Combined With a Fragrance Pulse Ejection System. Frontiers in Human Neuroscience, 14. https://doi.org/10.3389/fnhum.2020.523456

An older article from 2015 on scent and sniffing pleasant and unpleasant odors, noted that Autistics sniffed at pleasant and unpleasant odors with the same intensity whereas neurotypicals sniffed more intensely with pleasant odors and less intensely with unpleasant odors.
We wonder if the more intense sniff is increasing the intensity of the scent and thus contributing to increased sensory overwhelm to scent?
We would love to see some research into whether this could be developed into an easy intervention. We searched articles this week and could not find interventions but please let us know if there are some.
We would propose an intervention where Autistic children could learn to visually identify potentially unpleasant scents (this would need to be individually tailored) and also learn to control the intensity of their sniff to decrease the overwhelm. This could focus on scents that are more commonplace in everyday environments (schools, shops) and where the scent is impacting on occupations.
It has been difficult to research the olfactory (scent) sense in Autism, partly due to the difficulties with accuracy of measurement. A new precise and easy to use system has been developed – the odor pulse ejection system. It is described in this article:
This system was designed to more accurately measure olfactory processing including odor detection, identification and evaluation. Findings of the study using the odor pulse ejection system suggest differences in aspects of olfactory processing for autistics, including olfactory working memory and/or attention.
References
Article: a mechanistic link between Olfaction and Autism
Xu, M., Minagawa, Y., Kumazaki, H., Okada, K., & Naoi, N. (2020). Prefrontal Responses to Odors in Individuals With Autism Spectrum Disorders: Functional NIRS Measurement Combined With a Fragrance Pulse Ejection System. Frontiers in Human Neuroscience, 14. https://doi.org/10.3389/fnhum.2020.523456

Providing choice of menstrual products in Mental Health Unit Design
Sensory sensitivities are common in people with mental illness and Autistics and (1)
can impact on periods & menstrual products. This can include:
· touch
· visual input
· scent
· coordination and fine motor skills
· trauma
· pain and Interoception
· familiarity and uncertainty
Touch
When choosing menstrual products, there can be a variety of different preferences for touch sensations in menstrual products This includes the feeling of a tampon and cup (sometimes lubricant changes the dry tampon feeling) or the feeling of a bulky pad in underwear, or the feeling of the pad against the skin. If new to menstrual cycles it is useful to explore what option is the most comfortable. If the person has a preference then it is important to enable access to this preference. . When someone is sensitive to touch they can be unable to get used to (habituate) a sensation and this can be very irritating, distressing or overwhelming.

Sensory sensitivities are common in people with mental illness and Autistics and (1) can impact on periods & menstrual products. This can include:
· touch
· visual input
· scent
· coordination and fine motor skills
· trauma
· pain and Interoception
· familiarity and uncertainty
Touch
When choosing menstrual products, there can be a variety of different preferences for touch sensations in menstrual products This includes the feeling of a tampon and cup (sometimes lubricant changes the dry tampon feeling) or the feeling of a bulky pad in underwear, or the feeling of the pad against the skin. If new to menstrual cycles it is useful to explore what option is the most comfortable. If the person has a preference then it is important to enable access to this preference. . When someone is sensitive to touch they can be unable to get used to (habituate) a sensation and this can be very irritating, distressing or overwhelming.
Visual
Some people prefer not to see menstrual blood and may choose a product such as period underwear to be able to not sight it. If a person identifies that this is the case then it is trauma informed care to respect this.
Scent
Some people prefer not to smell menstrual blood and may choose a scent that masks the smell. Having access to this scent will be important for comfort.
Some people are sensitive to scents and will dislike a scented menstrual product. If they are sensitive to scent, they will be unable to get used to (habituate) to this scent.
Coordination and fine motor skills
Inserting a tampon or cup can require coordination and dexterity of hands and familiarity of their body. Even opening the packet can be tricky!
Trauma
A period or menstrual products can be a trauma trigger and using a particular menstrual product may be their preferred way of managing this trauma. Menstruation can sometimes result in dissociation or flashbacks.
Pain and Interoception
Some people experience severe pain with periods and may request medication to manage this. This can also be an opportunity to check if the person has discussed their period pain with their GP and to educate them on the possibility of endometriosis, if needed.
Joining in on walks or exercise programs may not be possible for someone who is having a heavy period, is dizzy or faint or in a lot of pain.
For people who are low in body awareness (Interoception) , it can be difficult to notice the sensations of a period starting, bloating, or the need to change a menstrual product.
Other factors impacting menstrual product choice
There can be other factors impacting on choice of menstrual products that are not for sensory reasons.
This can include
· Familiarity and uncertainty
· Transgender
Familiarity and uncertainty
Being in a mental health unit can be a very stressful time and it can be a time when someone does not want to try an unfamiliar menstrual product.
Transgender
Menstruation may trigger gender dysphoria for some transgender people. Other difficulties can include the lack of access to bins in mens toilets and heavily gendered menstrual products.
Accessing Menstrual products
To summarise, there are many reasons why someone may be requesting a particular menstrual product and providing a range of options can be very important to increase comfort and decrease distress. Some units have products available in
· Bathrooms
· Vending machines
· Shop/canteen on hospital premises (if they do not have a wide range then advocate to increase this).
Be mindful of how the person came into hospital. If they were unable to pack their bags they may not have been able to pack menstrual products. Most would have been in a highly stressed state and so may also have overlooked packing it.
Family members or friends may be able to bring preferred products to the unit. This may be useful to include in unit information eg brochures, website, noticeboards.
Some units require people to ask nurses for access to menstrual products. A discreet and private process to do this is preferable. There may also be a need to discreetly access clean sheets and towels, and cleaning products to soak/launder underwear or clothing.
The range of menstrual products includes:
· Tampons with or without applicator (cardboard applicators are available)
· Sports tampons
· Cups
· Pads, Liners
· Period underwear
· Menstrual sponges
· Tampons without string (google stringless tampons)
· Menstrual discs
· Access to free products if finances are limited
· Change of underwear
· Heat products to manage cramps eg electric hot water bottle
Another support that may be required for someone who is unwell, dissociated or sedated , may be to provide help to remind them to change products.
Health professionals’ discussions
This blog was inspired by an excellent article written by Hattie Porter in which they described the realities of trying to manage menstruation while in a mental health unit.
They recommend that health professionals on mental health and other hospital units:
· Discuss the availability of menstrual products on the wards. Are these freely available in bathrooms? Is there enough choice to meet each person’s needs?
· Discuss needs around menstruation (or menopause as relevant) in assessments.
· Provide easy access to choice of products to meet individual needs and preferences.
Other points
Mental Health Units that have limited access to menstrual products may be inspired to implement changes through the following points:
· If risk is a concern, consider that string on teabags is often allowed and is similar to tampon string. The risk is not considered to be so high that tampons are not allowed in a prison environment. However if this policy is in place, it is possible to use sponges and tampons without string as an alternative. For example https://www.beppy.com/en/beppy-tampons/
· WHO calls for menstrual health to be recognised, framed and addressed as a health and human rights issue, not a hygiene issue. More information is available in the reference section of this blog.
· The UK Home Office has a policy of free sanitary products to all female and transgender male prisoners to “help ensure menstruating detainees are “treated with dignity”.
Medical Conditions
Some people experience medical conditions that impact their experiences of menstruation. This includes:
· Heavy bleeding
· PCOS : Poly Cystic Ovary Syndrome
· Endometiriosis
· PMDD/PME Pre Menstrual Dysphoric Disorder/Premenstual Exacerbation
· Menopause
Universal Design
At Sensory Modulation Brisbane, we are calling for Universal Design in Mental Health Units for Sensory Sensitivities and this would include access to menstrual products that meet sensory and other preferences. There are other blog posts in this series eg reducing scents, sounds in mental health unit.
Sensory Modulation Brisbane also has recorded an online course which includes information on the importance of changing the environment in healthcare settings. (The webinar does not include further information on menstrual products) : tinyurl.com/4yz7hb4k
https://sensorymodulationbrisbane.ticketspice.com/sensory-modulation-using-a-sensory-lens-with-clients
Acknowledgement
Hattie Porter contributed to this article – thanks for your time, your words and your work in this area.
References and further information
Porter, Hattie, RCOT News “ It’s about bloody time we talk about periods” : https://www.rcot.co.uk/news/your-september-issue-otnews-0 or on twitter: @hat_teaa
World health organisation
https://www.who.int/news/item/22-06-2022-who-statement-on-menstrual-health-and-rights
WHO calls for menstrual Health to be recognized, framed and addressed as a health and human rights issue, not a hygiene issue:
WHO calls for three actions. Firstly, to recognize and frame menstruation as a health issue, not a hygiene issue – a health issue with physical, psychological, and social dimensions, and one that needs to be addressed in the perspective of a life course – from before menarche to after menopause. Secondly, to recognize that menstrual health means that women and girls and other people who menstruate, have access to information and education about it; to the menstrual products they need; water, sanitation, and disposal facilities; to competent and empathic care when needed; to live, study and work in an environment in which menstruation is seen as positive and healthy not something to be ashamed of; and to fully participate in work and social activities. Thirdly, to ensure that these activities are included in the relevant sectoral work plans and budgets, and their performance is measured.
UK Home Office
Britain said on Wednesday that it will provide free sanitary products to all female and transgender male prisoners to help ensure menstruating detainees are "treated with dignity".
The Home Office (interior ministry) said it would change the law to make it mandatory for police to ask every female detainee at the earliest opportunity if they need free pads or tampons.
All detainees will also be able to speak in private to a police staffer of the same sex about their health, welfare and hygiene needs, the government said.
The Home Office told the Thomson Reuters Foundation that transgender male detainees will also be able to request period products and speak privately to a staff member of a sex of their choosing.
"I have been clear that everyone who enters custody should be treated with dignity and have their personal needs met," Nick Hurd, minister for policing, said in a statement.
The Independent Custody Visiting Association (ICVA), which works to improve custody conditions, said some women had been stripped of all clothing, including underwear, and placed in paper suits in police cells without sanitary products.
Britain had about 3,760 female detainees in 2018 - who accounted for less than five percent of the total prison population - ministry of justice figures showed.
"These changes ensure that the needs of female detainees are addressed, that detainees have basic privacy to use a toilet and access to menstrual products and that dignity is promoted within the police custody environment," said ICVA's head Katie Kempen.
Period Poverty article
Period Poverty affects 500 million people world wide
https://www.medicalnewstoday.com/articles/period-poverty
Below, we list some period poverty statistics:
Globally, an estimated 500 millionTrusted Source people who menstruate lack access to menstrual products and hygiene facilities.
There are an estimated 16.9 million people who menstruate living in poverty in the United States.
A study involving college-aged individuals who menstruate reported that 14.2% had experienced period poverty in the past year. An additional 10.0% experienced it every month.
Research found that almost two-thirds of women in the U.S. with a low income could not afford menstrual products in the last year, while nearly half sometimes had to choose between buying food or menstrual products.

Sensory Assault
This blog is a commentary on a recent article by Beth Ohannesson Sarah Schoen, Vanessa Mitchell B Parent perspectives on children with sensory over-responsivity. The article describes a study in which parents of children with sensory over responsivity and sensory meltdowns/ sensory over responsivity episodes described their childrens description of the episodes and the strategies that they used to manage them.
This blog is a commentary on a recent article by Beth Ohannesson Sarah Schoen, Vanessa Mitchell B Parent perspectives on children with sensory over-responsivity. The article describes a study in which parents of children with sensory over responsivity and sensory meltdowns/ sensory over responsivity episodes described their childrens description of the episodes and the strategies that they used to manage them.
The parents were asked to discuss sensory meltdowns/ sensory over responsivity episodes with the children and to ask the children to describe how it felt.
The children described an intense sensory episode as:
· “It feels like knives are stabbing my bones,”
· “My whole body hurts,”
· “I'm so scared,”
· “You're killing me,”
· “It's painful.”
· A full description was obtained from one child's report, which included him saying: It’s painful, not physically, but it’s just too much. Don’t touch me, but don’t leave me, because it’s just too much. I’m so scared. There’s so much pressure that I have to go onto the ground. If you come over to comfort me, it’s killing me. I’m already down on the ground and now you’re killing me.
Other children indicated sensory specific reactions that included the following:
· “Sounds are too loud,”
· “Smells are too strong,”
· “It hurts my ears,”
· “Textures are too rough,”
· “It's completely overwhelming,”
· “I hate the feeling,”
· too many things are happening in my head and body at once, and it makes me mad.
The descriptions provided by the children resulted in a suggested change in the terminology or sensory meltdown/sensory over responsivity episode to better reflect the intensity of the experience. They proposed the term “sensory assault”. This term is more consistent with the literature linking physiological, neurologically driven adverse sensory experiences that activate autonomic nervous system fight, flight, or freeze response.
Julie and I and other OTs we have discussed this with, have heard similar descriptions from children and adults of the pain and distress of a Sensory Assault and the descriptions of overwhelming input. We will be interested to see whether this term becomes utilised in the OT literature.
In another part of the study , the families were asked to describe the strategies that they had used for the Sensory Assaults. This included:
· Stay with my child
· Gentle hold to keep everyone safe
· Give them proprioceptive input
· Name their feelings
· Other
· Yell
· Give them oral chewies or gum
· Countdown 5,4,3, 2 , 1
· Give consequences or withdraw a privilege
· Give time out.
The study includes the percentages that these strategies were used in a table form.
The majority of parents in the study were feeling frustrated that their efforts do not seem to help (n = 24, 66.7%) or feeling confused about how to help (n = 23, 63.6%). Parents also reported feeling hopeless about their efforts to help (n = 14, 38.9%) and angry at their child (n = 16, 44.4%). A minority (n = 11, 30.6%) of parents reported feeling confident when responding to their child during an SOR episode”.
It is interesting that none of the strategies were to reduce the overwhelming sensory input. At Sensory Modulation Brisbane, we recommend this as a first line strategy.
The full article is worth reading for the extra detail. and would love to see further research interviewing and expanding on the points raised in the article.
Sensory Assault Strategies
Sensory Modulation Brisbane suggested the following process in responding to a sensory assault
If possible, make changes to any sensory input in the environment
· Turn down lights (not complete darkness – just a lamp) and in particular fluorescent lights
· Use nil odour , or a fan or move away from intense scents
· Offer ear plugs, headphone to block sound or turn music down or move away from loud sounds.
· Remove any item of clothing or any item that may have a problematic texture
· Block any visual motion (eg cars, people walking by) by changing positioning or having someone else sitting or standing in the way of it.
Co-regulation
· Keep conversation to a minimum eg 5 word sentences. Person may have difficulty with processing speech or with speaking. For this reason, we advise not discussing the situation until later during a calm time. If they would like to speak and are unable to, use another communication strategy. If they are unfamiliar with not being able to speak, provide reassurance that this is short term and can occur during high distress.
· Provide a calming presence. Sit or stand beside the person quietly. Use strategies that you find calming for yourself.
· If the person is headbanging, or at risk of harming themselves then it is worthwhile discussing specific strategies with an OT.
Other calming sensory input
Any calming sensory input that is introduced needs to have been trialled previously and the person indicated that they like this input. During a Sensory Assault it is possible that the person does not want the sensory item and this needs to be respected. Also it is not uncommon for someone who has had a sensory assault to be irritable because of the intensity of what they have experienced
Calming input that may be useful includes:
· Backpack, bag, bag of rice on lap, blanket
· Heat /cold items (persons preference for temperature intensity)
· Drink of water. Small sips. May be hard to swallow*
· Tilting head down
· Rocking head and/or body rhythmically back and forth
· Moving/wiggling fingers and toes very slowly and gently
· Calming scent
· Swing
· Chewing items if they are not a risk if they are swallowed (*the person may have difficulty coordinating swallowing ).
· Using a single word or sound with a calm and long breath
Touching
· Some people like a strong hug, or touch.
· Pets can sometimes provide calming touch.
· Other people find that touch is too overwhelming during the experience. If you are unsure, it is preferable to not touch.
After the Sensory Assault
· Compete a Sensory Audit of the sensory input present during the Sensory Assault. A pdf of a Sensory Audit is available. This audit includes checking whether the person is in pain.
· Reflect/ or Ask the person who had the sensory assault to identify if they feel that any particular sensory input in the Sensory Assault was problematic. This is not possible with some people (eg due to age, cognition, dissociation etc) but is valuable information if available.
· Record the possible problematic sensory input and notice themes over time (be a sensory detective)
· Explore other options that may be useful during a sensory input and develop strategies to make sure that they are available eg sensory kit.
A sensory assault is a traumatic and distressing experience and individuals may express their distress through punching, headbanging, hair pulling, self harming, aggression, moaning. It is important to have a trauma informed perspective on this experience and to not engage in punishment or other behavioural responses. It may be useful to see an Occupational Therapist for more specific strategies
Training
The Sensory Modulation course describes sensory modulation strategies and the use of a sensory audit. The content can be generalised to apply to a range of situations. The course does not use the term Sensory Assault as it is new!
References
O’ Sullivan, J, Fitzgibbon, C (2017) Sensory Modulation Resource Manual
Beth Ohanneson, Sarah A. Schoen, Vanessa Mitchell (2023) Emerging Ideas. Parent perspectives on children with sensory over-responsivity Family Relations, Interdisciplinary Journal of Applied Family Science https://doi.org/10.1111/fare.12843
https://onlinelibrary.wiley.com/doi/10.1111/fare.12843
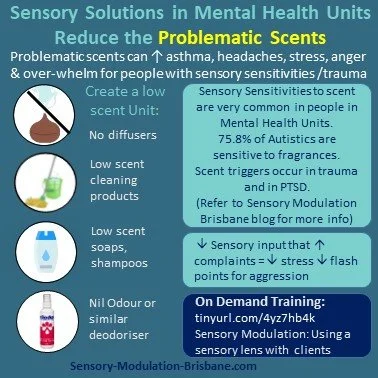
Low scent, fragrances in Mental Health Unit Design
The prevalence of fragrance sensitivities were investigated in the United States, United kingdom, Australia and Sweden by Steinemann (2019) and results included:
· 75.8% of Autistics are sensitive to fragrances
· 26% of the general population report being diagnosed with asthma/asthma like conditions and 57.8% are also fragrance sensitive.
Scents that were particularly problematic included:
· Air fresheners and deodorisers (54.8%)
· Being in a room with recently cleaned products (53.8%)
· Being near someone wearing a fragranced product (56.5%)

Low Scent, Fragrances in Mental Health Unit Design
This blog will outline the rationale for a low scent environment in Mental Health Units and offer recommendations with respect to the design of these environments.
People admitted to Mental Health inpatient Units present with a wide range of mental health disorders including schizophrenia, Borderline Personality Disorder, Post Traumatic Stress Disorder and Autism Spectrum Disorder. It is now understood that people with these diagnoses experience a higher rate of sensory sensitivities and other sensory processing challenges compared to the general population (Stromberg et al).
The prevalence of fragrance sensitivities were investigated in the United States, United kingdom, Australia and Sweden by Steinemann (2019) and results included:
· 75.8% of Autistics are sensitive to fragrances
· 26% of the general population report being diagnosed with asthma/asthma like conditions and 57.8% are also fragrance sensitive.
Scents that were particularly problematic included:
· Air fresheners and deodorisers (54.8%)
· Being in a room with recently cleaned products (53.8%)
· Being near someone wearing a fragranced product (56.5%)
There was a range of adverse health effects associated with fragranced product exposures for chemically sensitive individuals and this included:
· Respiratory problems (50.2%)
· Mucosal symptoms (39.4%)
· Migraine headaches (36.9%)
· Asthma attacks (25.2%)
Scent was identified as a barrier to engaging in occupations including:
· 37.4% are unable or reluctant to use public restrooms that have an air freshener, deodoriser or scented product.
· 51% enter a business but then leave as quickly as possible due to a fragranced product
· 9% of the general population has lost work days or lost a job in the past year due to illness from fragranced product exposure in the workplace
· 60% of students in one study had a physical reaction including headaches, shortness of breath, or a rash after being exposed to fragranced products. Additionally, 41% noted their reactions to fragranced products impacted their ability to concentrate on studying and taking exams. (Lee, 2019)
Healthcare
· 51.45% of the general population would prefer that healthcare facilities and healthcare professionals are fragrance free.
· 77.2% of Autistics would prefer fragrance free healthcare.
PTSD:
Herz (2021) found that odors may be the most incapacitating triggers for PTSD because:
“ (1) odors are invisible and there is often no way to prepare for or anticipate the possibility of exposure;
(2) odors evoke more emotional and evocative memories than other sensory stimuli
(3) odors are processed in the area of the brain where emotions, emotional memories, and associations are processed (the amygdala-hippocampal complex and orbitofrontal cortex), which comprises the same neural circuitry as PTSD due to their direct connection to the neural network of emotion, odors can instantly elicit affective responses and associations prior to and without cognitive appraisal That is, at-risk individuals are vulnerable to traumatic odor-triggered memories; odor processing inherently elicits highly emotionally charged memories; and, due to the automaticity of odor-evoked memories, encountering an odor associated with trauma can sideswipe cognitively prepared coping responses.
In addition to being highly insidious triggers, odors often play a central role in PTSD episodes. For example, in a report of 100 refugees who were seen at a psychiatric clinic, 45 percent reported experiencing an odor-triggered panic attack within the preceding month [51]. Odor cues can also trigger particularly negative flashbacks.”
Sensory Modulation Brisbane recommends that Mental Health Units respond to the needs of people with sensory sensitivities and trauma triggers to scents by implementing sensory modulation techniques and Universal Health Design features such as:
· Availability of Nil Odor, Stink Balm or other odor reducing strategies to provide an option for people to decrease a scent that they do not like.
· Providing personally preferred scent input eg options for different soaps, little containers with cotton balls and scent on it.
· Low scent cleaning , laundry and bathroom products
· No aromatherapy diffusers, incense etc
· Scents to be considered as a possible contributor for distress and agitation.
· Problem solving to address scents that are identified as problematic by people on the ward
· Designing spaces to separate the food areas to keep food scents in one location.
· Consideration of separate eating areas or other strategies for people with scent sensitivities or triggers or who need lower scent levels in order to comfortably eat.
· Healthcare professionals to wear low scent personal products.
· Air purifiers, plants
· Open windows and outdoor areas
· Completing a personal safety plan to identify useful and problematic scents
Further information on this topic is available on the On demand course:
References:
S. Herz R. Olfactory Virtual Reality: A New Frontier in the Treatment and Prevention of Posttraumatic Stress Disorder. Brain Sciences. 2021; 11(8):1070. https://doi.org/10.3390/brainsci11081070
Lee, R., Westmoreland, D., Maju, M., Apolloni, A., Bullock, H., Wang, A., & Sidhu, S. (2019, November). Assessing the Prevalence of Chemical Sensitivities to Fragranced Products Among Undergraduate Students & Its Impact on Educational Experiences. In APHA's 2019 Annual Meeting and Expo (Nov. 2-Nov. 6). APHA.
Sensory Modulation Resource Manual
Steinemann, A. International prevalence of chemical sensitivity, co-prevalences with asthma and autism, and effects from fragranced consumer products. Air Qual Atmos Health 12, 519–527 (2019). https://doi.org/10.1007/s11869-019-00672-1
https://link.springer.com/article/10.1007/s11869-019-00672-1
Steinemann, A. The fragranced products phenomenon: air quality and health, science and policy. Air Qual Atmos Health 14, 235–243 (2021). https://doi.org/10.1007/s11869-020-00928-1
https://link.springer.com/article/10.1007/s11869-020-00928-1#citeas
Maria Strömberg, Lina Liman, Peter Bang, and Kajsa Igelström.Experiences of Sensory Overload and Communication Barriers by Autistic Adults in Health Care Settings.Autism in Adulthood.Mar 2022.66-75.http://doi.org/10.1089/aut.2020.0074
https://www.abc.net.au/news/2023-01-09/too-many-smelly-candles-here-s-how-scents-impact-the-air-quality/101823806

Therapy rooms and waiting rooms: designing for sensory needs
At Sensory Modulation Brisbane, we have been advocating for Universal Design in Mental Health Units for Sensory Sensitivities and we would recommend that this is expanded to therapy rooms, waiting rooms and all health care spaces.
Many people who attend Therapy practices have sensory processing patterns that are more sensitive, more avoiding, or more seeking or more missing of sensations than others and this can vary between different senses. This includes:
· Autistics have sensory processing differences recognised as a diagnostic criteria. (DSM5)
· People with PTSD often have reactivity and hypervigilance to certain sensations
· People with schizophrenia often have auditory processing and visual perception challenges.
· ADHDers frequently have sensory processing differences (Schulze 2020)
· A high percentage of people with mental illness have interoceptive difficulties
Therapy room with grey lounge, green cushions, a white blanket and a plant on a small table. We would remove the aromatherapy sticks though!
At Sensory Modulation Brisbane, we have been advocating for Universal Design in Mental Health Units for Sensory Sensitivities and we also recommend this for therapy rooms, waiting rooms and all health care spaces.
Many people who attend Therapy practices have sensory processing patterns that are more sensitive, more avoiding, or more seeking or more missing of sensations than others and this can vary between different senses. This includes:
· Autistics have sensory processing differences recognised as a diagnostic criteria. (DSM5)
· People with PTSD often have reactivity and hypervigilance to certain sensations
· People with schizophrenia often have auditory processing and visual perception challenges.
· ADHDers frequently have sensory processing differences (Schulze 2020)
· A high percentage of people with mental illness have interoceptive difficulties
It can be useful to design for people with sensory sensitivities as it is easier to add sensory input if needed rather than take it away.
Lighting
· Ideally a dimmable light that is set at the preference level of an individual client
· Curtains or Blinds to block out light
· If there is a florescent light, turn it off and use lamps instead.
Sound
· Improving office acoustics can be very beneficial for everyone in terms of privacy and also reducing distractions and sensory sensitivities and overload.
· It is preferable to not use music in a waiting room environment as people who want music can usually access this on their phone.
Scent
· Scents can be a trauma trigger, allergy trigger or lead to sensory sensitivity and overload. So having a low scent therapy room and waiting room can be very important. For this reason, we do not recommend diffusers in public spaces.
· Sometimes it may be necessary to neutralise odours. Try nil odour drops.
Interoception needs
Sometimes therapy is the place where people relax a little and notice that they need to go to the toilet, drink some water or have some snacks. They may not have noticed these interoceptive needs earlier. Close proximity to toilets, water and food can be useful.
Comfortable Seating
There are many people in pain or who have hypermobility and are attending therapy offices. Comfortable seating can make a big difference.
Calming tools
At Sensory Modulation Brisbane, our favourite sensory tools for offices including a weighted cushion, a box of fidgets, icy water or ice packs and invitations to reduce the lighting or turn on or off the pink/brown/white noise machine.
Visual Movement
Ideally design waiting rooms so that there is not a lot of visual movement eg people walking past, traffic etc. Or provide options to be able to not face this visual movement.
Clear Pathways
It is useful for pathways to be clear and obvious and for signage to be clear. It can also be useful to take pictures of landmarks and have this available on website or new starter information .
Personal preferences
It can be useful to invite individuals to use their preferred fidgets, earplugs, sunglasses, back cushion etc so that they are comfortable
Nature
Access to nature can be calming. A plant or a picture of nature can be good additions to an office
Previous blog posts have discussed changing sensory input within a psychiatric hospital:
Training:
https://sensorymodulationbrisbane.ticketspice.com/sensory-modulation-using-a-sensory-lens-with-clients
References:
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Marcel Schulze, Silke Lux, Alexandra Philipsen et al. Sensory Processing in Adult ADHD – A Systematic Review, 10 September 2020, PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-71514/v1]
chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://assets.researchsquare.com/files/rs-71514/v1/d616340b-9b38-4732-b56f-7c249e0632f7.pdf?c=1631855030
Sugiyama, S., et al(2021). The Auditory Steady-State Response: Electrophysiological Index for Sensory Processing Dysfunction in Psychiatric Disorders. Frontiers in psychiatry, 12, 644541.
Sensory Modulation Resource Manual

Sensory Kits , Trauma Informed Practice and NDIS
Using Sensory items to calm and ground are recognized evidence based strategies.
Yet some people in the NDIS scheme are having NDIS Plan Managers refuse to fund sensory items
This blog provides a rationale for the NDIS to make changes to their website and price guide based on two guidelines.
1. The Disability Guidelines for Trauma –Informed Practice: Supporting people with disability who have experienced complex trauma
2. NDIS Quality and Safeguards Commission (2020) Regulated Restrictive Practices Guide

Using Sensory items to calm and ground are recognized evidence based strategies.
Yet some people in the NDIS scheme are having NDIS Plan Managers refuse to fund sensory items
This blog provides a rationale for the NDIS to make changes to their website and price guide based on two guidelines.
1. The Disability Guidelines for Trauma –Informed Practice: Supporting people with disability who have experienced complex trauma
2. NDIS Quality and Safeguards Commission (2020) Regulated Restrictive Practices Guide
The Disability Guidelines for Trauma-Informed Practice: Supporting people with disability who have experienced complex trauma were developed in response to the disability royal commissions findings of high numbers of cases of abuse against people with disability. In response, the government provided funding for the project to develop the Disability Guidelines for Trauma-Informed Practice:
“The Morrison government is backing the creation of a best-practice guide to help the disability sector better support people with disability who have experienced complex trauma.
Social Services Minister Anne Ruston said the government was investing $267,760 in the project to ensure Australia leads the way in supporting people with disability who suffer violence, abuse, neglect or exploitation.
“The Morrison government will fund Blue Knot Foundation to guide organisations and practitioners on how to better understand complex trauma and deliver trauma-informed care to the disability community,” Ruston said.”
(Probono Australia) https://probonoaustralia.com.au/news/2020/08/new-guide-to-help-build-a-trauma-informed-disability-sector/
Within the Disability Guidelines for Trauma-Informed Practice , there is a section on developing comfort kits:
“Before the person needs grounding and if the person is able:
• Locate something that the person finds calming to look at.
• Locate something that the person finds calming to listen to.
• Locate something that the person likes to touch.
• Locate something that the person likes to smell.
• Locate something that the person likes to taste.
Place all of these items in a box. When triggered encouraged the person to access their box and use the five senses to explore each item until they can return to the Window of Tolerance.”
If a person is in the Window of Tolerance it means that they are able to concentrate and engage in activities. (Being outside the window of tolerance includes being stressed or shutdown)
Another guideline which is also supportive of developing comfort kits and sensory items is the NDIS Quality and Safeguards Commission (2020) Regulated Restrictive Practices Guide.
Examples of using sensory items to calm include:
Participant “having a quiet space in her home with sensory and relaxation items”. P 38
Participant having a sensory room that was designed for her sensory needs. “this included different items and activities, some of which were portable and could be used within the community when she needed them……The sensory room was to be used proactively to assist Emma to feel calm when she was beginning to show early signs of distress. P 55 and 56
Despite these guidelines having clear support for the provision of sensory items for people with disabilities, it is something that many participants find that it is difficult to obtain funding for.
Solution: NDIS to change the " would we fund it page" and/or develop a line item in their price guide to support people with disabilities and trauma

Using alternatives to torch light monitoring in Mental Health Unit Design
This blog will outline some of the challenges involved in using torch light to observe clients in mental health units at night and also provide some alternative options. Part of routine mental health care on mental health units is regular observations of people while they are sleeping/lying in bed. These routine observations are undertaken due to their perceived benefit in ensuring safety and wellbeing and to reduce the risk of suicide or severe harm. Nursing staff may need to complete observations up to 4 times per hour overnight and torch light is frequently used.

This blog will outline some of the challenges involved in using torch light to observe clients in mental health units at night and also provide some alternative options. Part of routine mental health care on mental health units is regular observations of people while they are sleeping/lying in bed. These routine observations are undertaken due to their perceived benefit in ensuring safety and wellbeing and to reduce the risk of suicide or severe harm. Nursing staff may need to complete observations up to 4 times per hour overnight and torch light is frequently used.
Veale et al (2019) researched the lived experience of these observations and found that these observations interrupted sleep through the torch light, sounds of staff opening and closing bedroom doors and staff talking to each other. People also reported that they found having somebody enter the room in the middle of the night intimidating and unsettling. For many people, this interruption can then make it difficult to return to sleep.
Improving sleep quality on mental health units is important to improve mental health and reduce suicide risk and decrease use of hypnotic medications. (Gardiner 2022) Improving sleep quality has been found to reduce aggressive incidents for psychiatric inpatients residing in secure facilities such as forensic psychiatric hospitals. (Van Veen et al 2020)
Alternatives to torch light that have been discussed have included remote monitoring systems, location trackers and video trackers. The majority of people found the remote monitoring systems acceptable (Veale et al 2019) but the location tracking and video monitoring have been identified as unsuitable due to privacy concerns. (Guardian, 2022)
Sensory Modulation Brisbane has identified the following remote monitoring systems as possible options to replace torch light observations:
At Sensory Modulation Brisbane, we are calling for Universal Design in Mental Health Units for Sensory Sensitivities and this would include replacing torch light observations. The rationale is that so many mental health diagnoses have people with sensory sensitivities. This would also assist Autistics who were on mental health units. People with other sensory processing preferences could also be catered for through adding in personally preferred input from a base of catering for sensory sensitivities.
Sensory Modulation Brisbane also has recorded an online course which includes information on the importance of changing the environment in healthcare settings: tinyurl.com/4yz7hb4k
https://sensorymodulationbrisbane.ticketspice.com/sensory-modulation-using-a-sensory-
lens-with-clients
#Universaldesigninmentalhealthunitssensorysensitivities #sensory #mental health #autistic #mentalhealth_community #schizophrenia #sensoryprocessingawareness #sensoryprocessingsensitivity #psychiatric #occupationaltherapy
More Information:
“This paper argues that intermittent nursing observations of in-patients at night do not reduce the risk of suicide or severe self-harm. Suicides between 23.00 h and 07.00 h are rare, and these overwhelmingly occur under intermittent observations. Such observation is purely a defensive intervention to document that a patient is safe at a particular time, as there is no engagement. For the large majority of in-patients, it has the unintended consequence of causing sleep deprivation. The intervention may cause harm to in-patients by making their disorder worse and increase their risk during the day. If patients are judged to be at immediate risk, then they should be placed on constant observation. If they are not, then optimising sleep is important for treating a psychiatric disorder and they should be placed on general observations.”
Veale D. Against the stream: intermittent nurse observations of in-patients at night serve no purpose and cause sleep deprivation. BJPsych Bull. 2019 Aug;43(4):174-176. doi: 10.1192/bjb.2018.116. Epub 2019 Feb 11. PMID: 30739621; PMCID: PMC6642991
“For psychiatric inpatients residing in secure facilities such as forensic psychiatric hospitals, worse sleep quality and higher insomnia scores significantly relate to aggression, hostility and violent incidents (Kamphuis et al., 2014). Thus, targeting inpatient sleep quality can help to reduce aggressive incidents in these populations, which is paramount to continued successful psychiatric treatment (Van Veen et al., 2020).”
Maaike M. Van Veen, Julie Karsten, Robbert-Jan Verkes & Marike Lancel (2020) Sleep quality is associated with aggression in forensic psychiatric patients, independent of general psychopathology, The Journal of Forensic Psychiatry & Psychology, 31:5, 699-713, DOI: 10.1080/14789949.2020.1785526
“A systematic search of the literature on the environment and nursing observations at night revealed few studies conducted on a psychiatric ward. A meta-analysis identifies the problems of sleep deprivation through noise on medical wards (DuBose & Hadi, 2016). There are also studies identifying that the large majority of psychiatric inpatients experience insomnia without focusing on the determinants”.
(Haynes, Parthasarathy, Kersh, & Bootzin, 2011; Horne, Hay, Watson, & Anderson, 2018; Keeley, 2010; Muller, Olschinski, Kundermann, & Cabanel, 2016). Improving sleep is important because sleep deprivation makes a psychiatric disorder worse (Krystal, 2012) and increases the risk of suicide (Malik et al., 2014).
“Importantly, sleep duration is negatively correlated with subsequent length of time in hospital (Langsrud, Vaaler, Kallestad, & Morken, 2016). The treatment of insomnia has been shown to lessen psychotic experiences (Freeman et al., 2017), mania, (Harvey et al., 2015), depression and anxiety (Ye et al., 2015).”
Veale, D., Sabriha, A., Pagageorgio, A., Gornay, K (2019) The psychiatric ward environment and nursing observations at night: A qualitative study VL - 27 DO - 10.1111/jpm.12583 JO -Journal of Psychiatric and Mental Health Nursing
“Another procedure of which all patients expressed an overall disapproval was the use of light during night observations. They reported being severely disturbed by the use of torches or by bedroom lights being turned on without warning.
“I probably didn’t really go to sleep. They kept coming in every 15 minutes. Sometimes they turn the florescent room lights on in the night, that’s horrible. They would turn the light on until I made some movement or showed I am ok. Sometimes they would use torches as well but better than lights being turned on. (Participant 1)
“Descriptions of night observations were always followed by a reference by the interviewee to the negative impact it had on their emotional state. In some patients, this contributed to a constant state of anxiety and a feeling of being unsettled.”
“The nurses try to use a lower voltage bulb in an attempt not to startle you. But when the room is dark to begin with any light looks so bright. (Participant 6) “
“Startling is when they come in and I see a silhouette, it really frightens me! (Participant 7)”
“At the end of each interview, participants were encouraged to provide their feedback regarding practices that might improve disturbances in night wards. Suggestions in respect to minimizing light disturbances included the use of night-vision glasses or a CCTV camera (only during night-time). Concerning the reduction of noise, suggestions included the following: installing floor coverings, using soft closing doors or applying foam to the doors to soundproof them. Recommendations for safety concerns included the installation of an alarm in the bedroom and for privacy concerns, neon gas windows which could be controlled by both staff members and patients.”
Veale D. Against the stream: intermittent nurse observations of in-patients at night serve no purpose and cause sleep deprivation. BJPsych Bull. 2019 Aug;43(4):174-176. doi: 10.1192/bjb.2018.116. Epub 2019 Feb 11. PMID: 30739621; PMCID: PMC6642991.
Barrera A, Gee C, Wood A, Gibson O, Bayley D, Geddes J. Introducing artificial intelligence in acute psychiatric inpatient care: qualitative study of its use to conduct nursing observations. Evid Based Ment Health. 2020 Feb;23(1):34-38. doi: 10.1136/ebmental-2019-300136. Erratum in: Evid Based Ment Health. 2021 May;24(2): PMID: 32046991; PMCID: PMC7034347.
Poppy May Gardiner, Florence-Emilie Kinnafick, Kieran C. Breen, Alessandra Girardi & Iuliana Hartescu (2022) Behavioural, medical & environmental interventions to improve sleep quality for mental health inpatients in secure settings: a systematic review & meta-analysis, The Journal of Forensic Psychiatry & Psychology, 33:5, 745-779, DOI: 10.1080/14789949.2022.2111320
https://www.tandfonline.com/doi/full/10.1080/14789949.2022.2111320
“NHS trust criticised over system that films mental health patients in their bedroom “ The Guardian, 2022 https://www.theguardian.com/society/2021/dec/13/nhs-trusts-urged-to-ditch-oxevision-system-covert-surveillance-mental-health-patients
https://www.nsw.gov.au/news/trial-of-pulse-monitoring-for-suicide-prevention
Experience of night environment on the ward survey https://onlinelibrary-wiley-com.ezproxy.library.uq.edu.au/doi/full/10.1111/jpm.12583
This survey may be useful to gather data for pre-post intervention changing the torch light
on the wards.
“The categories identified were used to develop a questionnaire to monitor the ward environment and impact of observations at night (Appendix 2). This could be used in a Quality Improvement Project to improve the quality of sleep on a ward. Ideally, the questionnaire would be used in conjunction with a light and decibel metre and measure of sleep quality to obtain more accurate estimations about the ward environment at night.”
Veale, D., Sabriha, A., Pagageorgio, A., Gornay, K (2019) The psychiatric ward environment and nursing observations at night: A qualitative study VL - 27 DO - 10.1111/jpm.12583 JO - Journal of Psychiatric and Mental Health Nursing